

Type XXII Collagen Complements Fibrillar Collagens in the Serological Assessment of Tumor Fibrosis and the Outcome in Pancreatic Cancer
- PMID: 36497023
- PMCID: PMC9738409
- DOI: 10.3390/cells11233763
Type XXII Collagen Complements Fibrillar Collagens in the Serological Assessment of Tumor Fibrosis and the Outcome in Pancreatic Cancer
Abstract
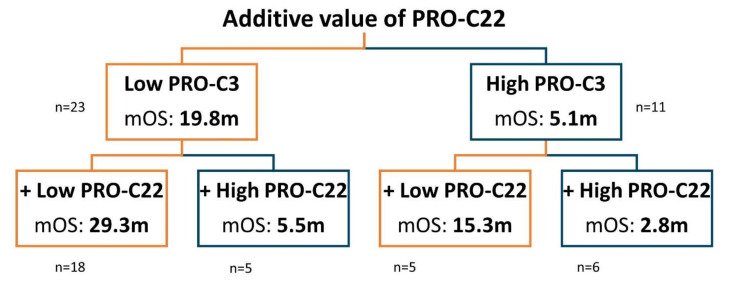
Circulating fragments of type III collagen, measured by PRO-C3, has shown promising results as a tumor fibrosis biomarker. However, the fibrotic tumor microenvironment consists of many other collagens with diverse functions and unexplored biomarker potential. One example hereof is type XXII collagen (COL22). In this study, we investigated the biomarker potential of COL22 by measuring this in serum. An ELISA, named PRO-C22, was developed and measured in two serum cohorts consisting of patients with various solid tumors (n = 220) and healthy subjects (n = 33) (Cohort 1), and patients with pancreatic ductal adenocarcinoma (PDAC) (n = 34), and healthy subjects (n = 20) (Cohort 2). In Cohort 1, PRO-C22 was elevated in the serum from patients with solid tumors, compared to healthy subjects (p < 0.01 to p < 0.0001), and the diagnostic accuracy (AUROC) ranged from 0.87 to 0.98, p < 0.0001. In Cohort 2, the high levels of PRO-C22, in patients with PDAC, were predictive of a worse overall survival (HR = 4.52, 95% CI 1.90−10.7, p = 0.0006) and this remained significant after adjusting for PRO-C3 (HR = 4.27, 95% CI 1.24−10.4, p = 0.0013). In conclusion, PRO-C22 has diagnostic biomarker potential in various solid tumor types and prognostic biomarker potential in PDAC. Furthermore, PRO-C22 complemented PRO-C3 in predicting mortality, suggesting an additive prognostic value when quantifying different collagens.
Keywords: ECM; PDAC; collagens; non-invasive biomarker; tumor fibrosis; type XXII collagen.
Conflict of interest statement
A patent has been filed for the PRO-C22 ELISA. E.A.M., J.T.-U., C.J., N.I.N., M.A.K. and N.W. are employed at Nordic Bioscience A/S, a biotech company involved in the discovery and development of blood-based biomarkers. I.M.C., J.S.J., H.M.H.D., L.N.J. and C.P.H., have no conflict of interest to declare. E.A.M., M.A.K. and N.W. own stock in Nordic Bioscience A/S.
Figures





Similar articles
-
High serum levels of the C-propetide of type V collagen (PRO-C5) are prognostic for short overall survival in patients with pancreatic ductal adenocarcinoma.Front Mol Biosci. 2023 Mar 10;10:1158058. doi: 10.3389/fmolb.2023.1158058. eCollection 2023. Front Mol Biosci. 2023. PMID: 36968276 Free PMC article.
-
Type XX Collagen Is Elevated in Circulation of Patients with Solid Tumors.Int J Mol Sci. 2022 Apr 8;23(8):4144. doi: 10.3390/ijms23084144. Int J Mol Sci. 2022. PMID: 35456962 Free PMC article.
-
Noninvasive prognostic biomarker potential of quantifying the propeptides of Type XI collagen alpha-1 chain (PRO-C11) in patients with pancreatic ductal adenocarcinoma.Int J Cancer. 2021 Jul 1;149(1):228-238. doi: 10.1002/ijc.33551. Epub 2021 Mar 22. Int J Cancer. 2021. PMID: 33687786
-
Fibrotic activity quantified in serum by measurements of type III collagen pro-peptides can be used for prognosis across different solid tumor types.Cell Mol Life Sci. 2022 Mar 25;79(4):204. doi: 10.1007/s00018-022-04226-0. Cell Mol Life Sci. 2022. PMID: 35332383 Free PMC article. Review.
-
Dkk1 involvement and its potential as a biomarker in pancreatic ductal adenocarcinoma.Clin Chim Acta. 2019 Jan;488:226-234. doi: 10.1016/j.cca.2018.11.023. Epub 2018 Nov 16. Clin Chim Acta. 2019. PMID: 30452897 Review.
Cited by
-
Revisiting Circulating Extracellular Matrix Fragments as Disease Markers in Myelofibrosis and Related Neoplasms.Cancers (Basel). 2023 Aug 29;15(17):4323. doi: 10.3390/cancers15174323. Cancers (Basel). 2023. PMID: 37686599 Free PMC article. Review.
-
Preliminary investigation of elevated collagen and blood-clotting markers as potential noninvasive biomarkers for small cell lung cancer.Thorac Cancer. 2023 Oct;14(28):2830-2838. doi: 10.1111/1759-7714.15066. Epub 2023 Aug 19. Thorac Cancer. 2023. PMID: 37596821 Free PMC article.
-
Collagen in pituitary adenomas: A comprehensive review of biological roles and clinical implications.J Clin Transl Endocrinol. 2025 Jul 10;41:100408. doi: 10.1016/j.jcte.2025.100408. eCollection 2025 Sep. J Clin Transl Endocrinol. 2025. PMID: 40697902 Free PMC article. Review.
-
High serum levels of the C-propetide of type V collagen (PRO-C5) are prognostic for short overall survival in patients with pancreatic ductal adenocarcinoma.Front Mol Biosci. 2023 Mar 10;10:1158058. doi: 10.3389/fmolb.2023.1158058. eCollection 2023. Front Mol Biosci. 2023. PMID: 36968276 Free PMC article.
-
Collagen formation, function and role in kidney disease.Nat Rev Nephrol. 2025 Mar;21(3):200-215. doi: 10.1038/s41581-024-00902-5. Epub 2024 Nov 15. Nat Rev Nephrol. 2025. PMID: 39548215 Review.
References
-
- WHO WHO|Cancer Factsheet. [(accessed on 23 July 2021)]; Available online: http://www.who.int/mediacentre/factsheets/fs297/en/
-
- World Health Organization . WHO Report on Cancer: Setting Priorities, Investing Wisely and Providing Care for All. World Health Organization; Geneva, Switzerland: 2020.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
