

Tumor Location and a Tumor Volume over 2.8 cc Predict the Prognosis for Japanese Localized Prostate Cancer
- PMID: 36497304
- PMCID: PMC9740872
- DOI: 10.3390/cancers14235823
Tumor Location and a Tumor Volume over 2.8 cc Predict the Prognosis for Japanese Localized Prostate Cancer
Abstract
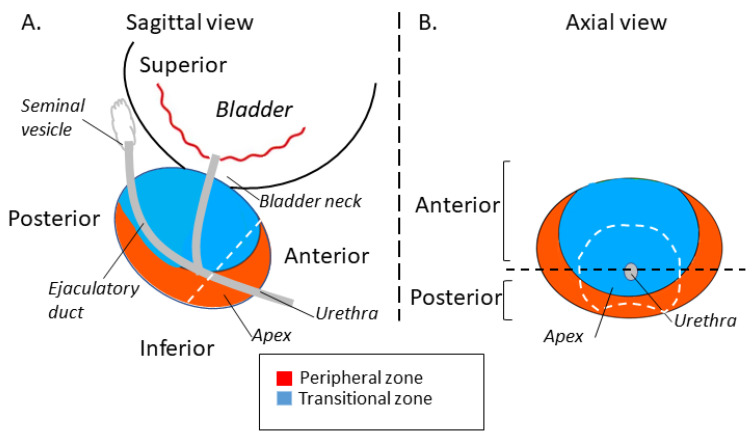
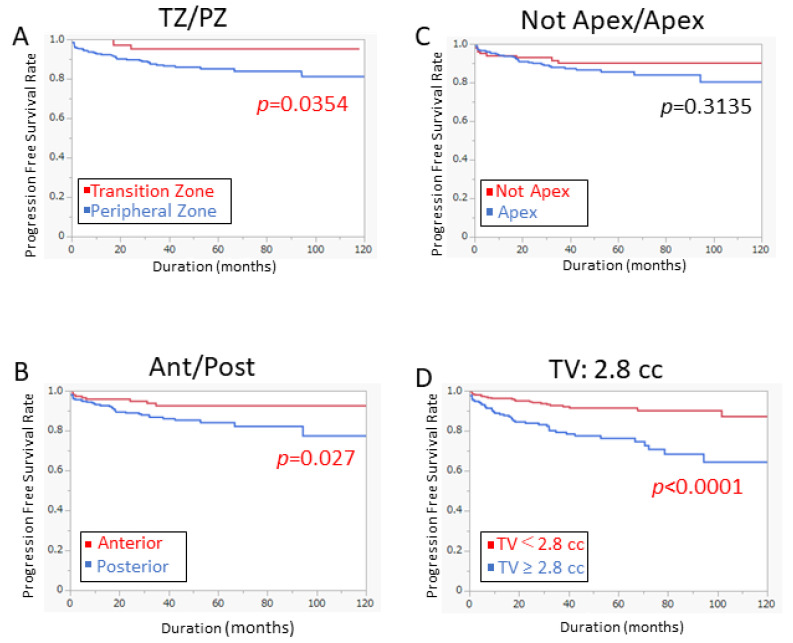
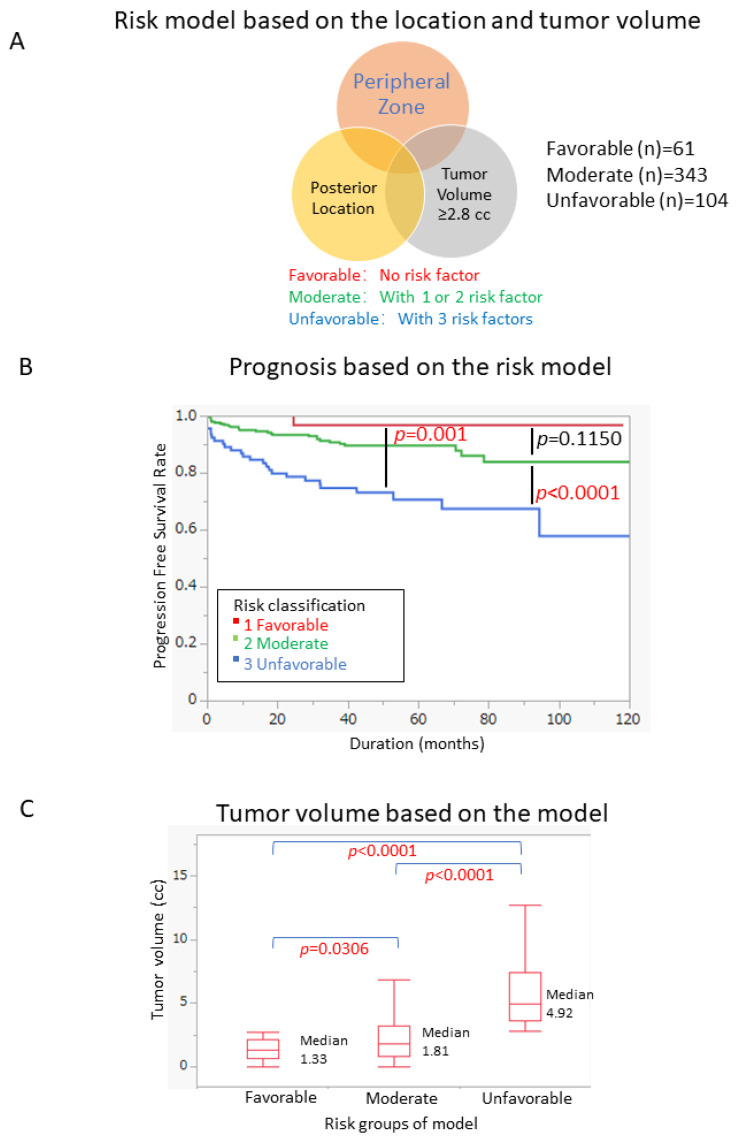
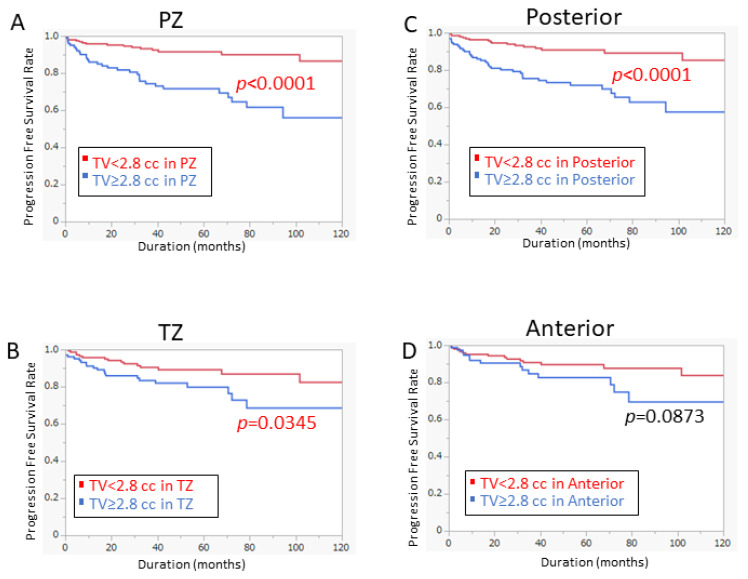
(1) Objective: Our study investigated the prognostic value of tumor volume and location in prostate cancer patients who received radical prostatectomy (RP). (2) Methods: The prognostic significance of tumor volume and location, together with other clinical factors, was studied using 557 patients who received RP. (3) Results: The receiver operating characteristic (ROC) curve identified the optimal cutoff value of tumor volume as 2.8 cc for predicting biochemical recurrence (BCR). Cox regression analysis revealed that a tumor in the posterior area (p = 0.031), peripheral zone (p = 0.0472), and tumor volume ≥ 2.8 cc (p < 0.0001) were predictive factors in univariate analysis. After multivariate analysis, tumor volume ≥ 2.8 cc (p = 0.0225) was an independent predictive factor for BCR. Among them, a novel risk model was established using tumor volume and location in the posterior area and peripheral zone. The progression-free survival (PFS) of patients who met the three criteria (unfavorable group) was significantly worse than other groups (p ≤ 0.001). Furthermore, multivariate analysis showed that the unfavorable risk was an independent prognostic factor for BCR. The prognostic significance of our risk model was observed in low- to intermediate-risk patients, although it was not observed in high-risk patients. (4) Conclusion: Tumor volume (≥2.8 cc) and localization (posterior/peripheral zone) may be a novel prognostic factor in patients undergoing RP.
Keywords: biochemical recurrence; prognostic factor; prostate cancer; tumor location; tumor volume.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Everist M.M., Howard L.E., Aronson W.J., Kane C.J., Amling C.L., Cooperberg M.R., Terris M.K., Freedland S.J. Socioeconomic status, race, and long-term outcomes after radical prostatectomy in an equal access health system: Results from the SEARCH database. Urol. Oncol. 2019;37:289.e11–289.e17. doi: 10.1016/j.urolonc.2018.12.004. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
