

Schober Test and Its Modifications Revisited-What Are We Actually Measuring? Computerized Tomography-Based Analysis
- PMID: 36498470
- PMCID: PMC9736537
- DOI: 10.3390/jcm11236895
Schober Test and Its Modifications Revisited-What Are We Actually Measuring? Computerized Tomography-Based Analysis
Abstract
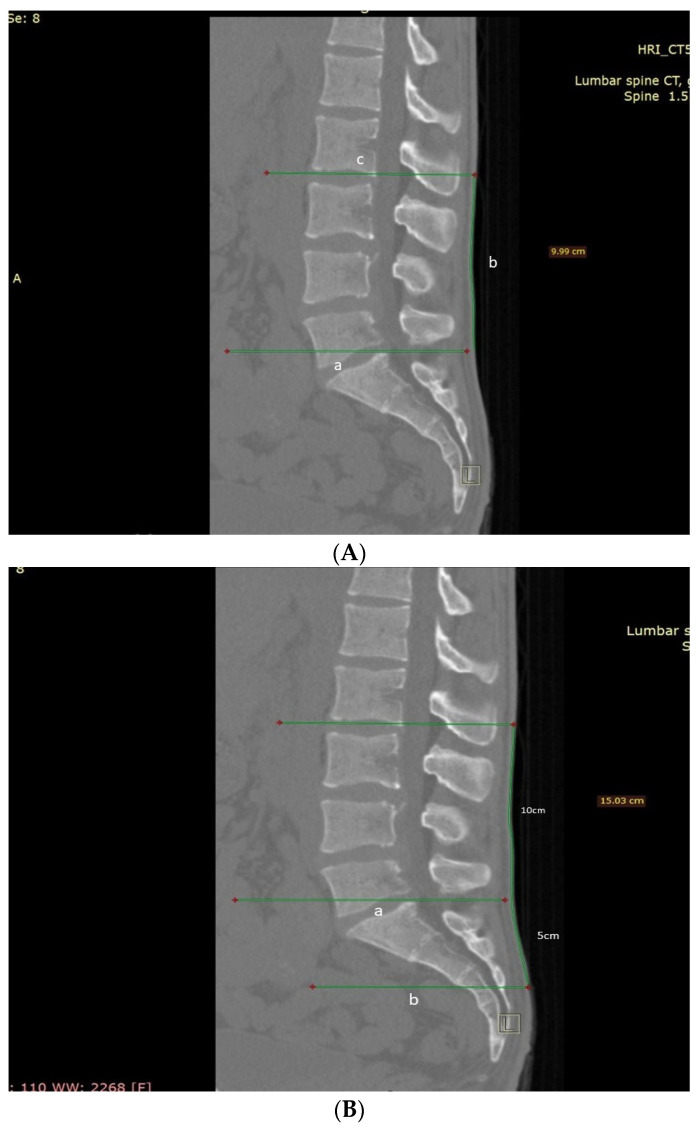
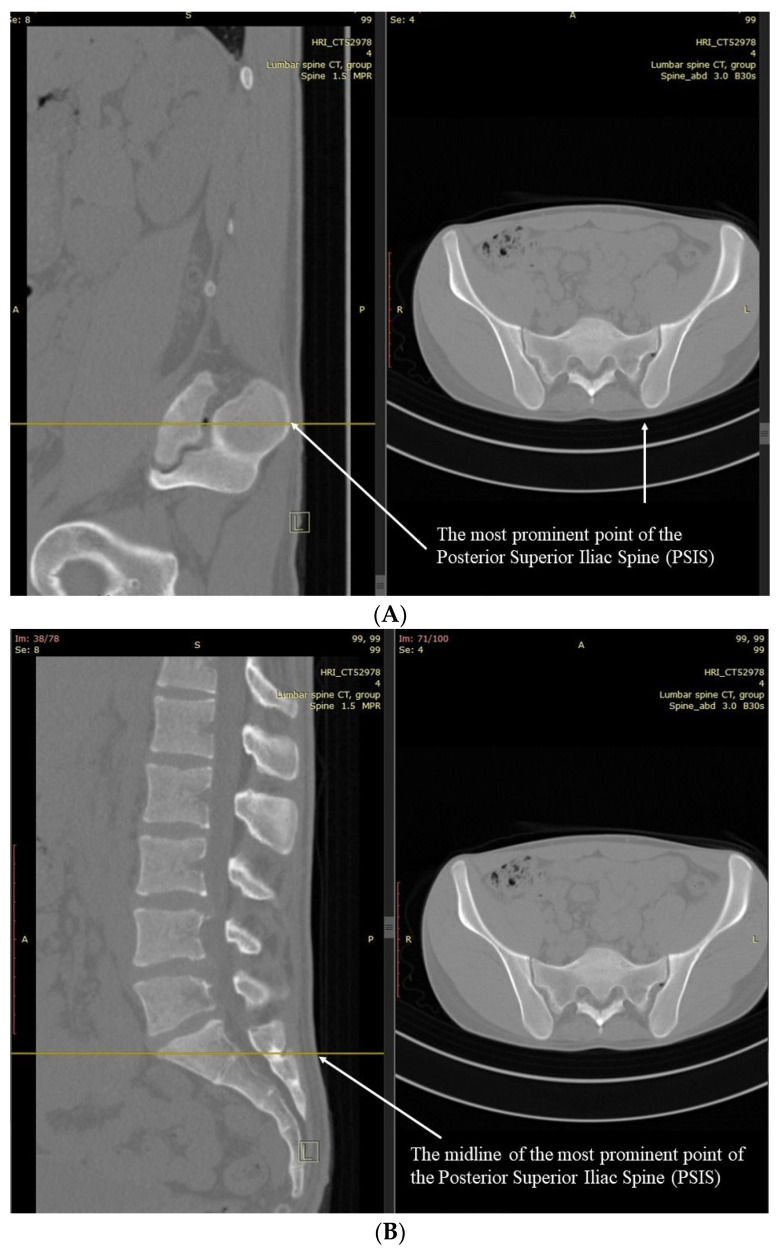
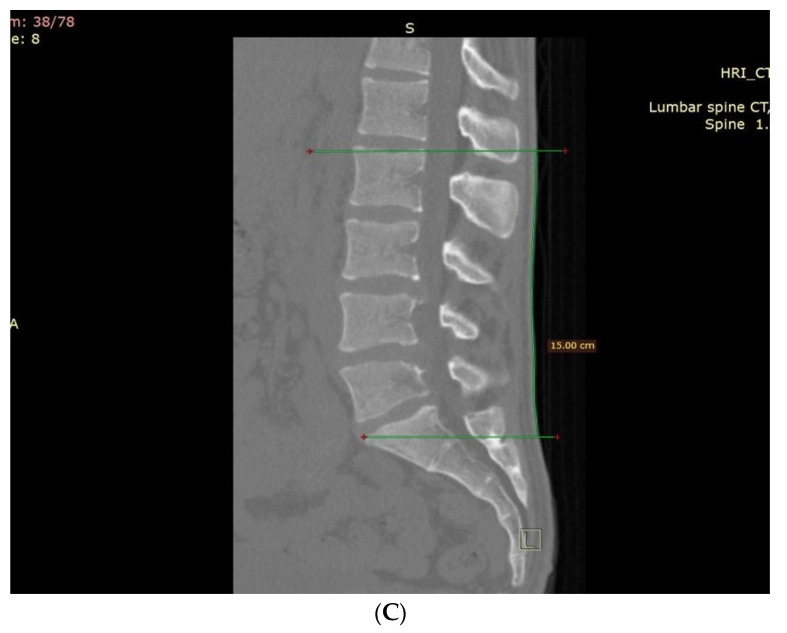
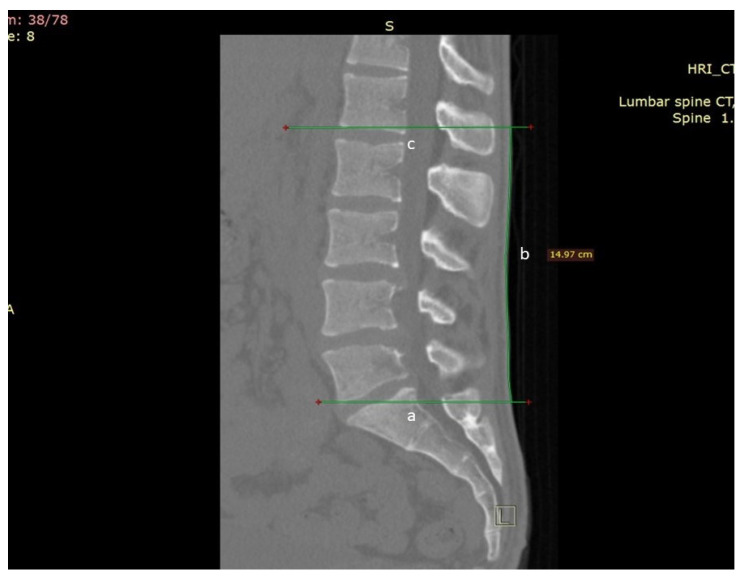
Objective: Examine Schober test's (ST), Modified ST (MST), and Modified-Modified ST (MMST) surface markers' accuracy in spanning lumbar L1-S1 motion segments and repeatability related to actual patient anatomy as measured on sagittal CT scans.
Methods: The study included 25 patients of varying heights, weights, and gender without prior spinal surgery or deformity. Researchers assessed patients' CT scans for ST, MST, and MMST skin levels of the measured cephalic and caudal endpoints.
Results: The original ST failed to include at least one lumbar motion segment in all patients, omitting the L1-L2 motion segment in 17 patients and the L2-L3 in another eight. The additional cephalic length of the MST did not improve the inclusion of the actual L1-S1 components. The MMST measured 19 'patients' entire L1-S1 motion segments, reaching a 76% accuracy rate. WMST, measuring 16 cm (instead of MMST's 15 cm), improved the measurement significantly, measuring the L1-S1 motion segments in all cases (with 100% accuracy).
Conclusion: ST and its modifications fail to span the L1-S1 motion segments and are thus prone to underestimating lumbar spine motion. This study shows that the WMST is much more accurate than previous modifications and is a better tool for evaluating lumbar spine motion.
Keywords: Schober test; lumbar; modified; range of motion.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Lotan R., Smorgick Y., Anekstein Y., Rudik O., Prosso I., Hershkovich O. Kyphoplasty for Elderly Patients with Vertebral Compression Fractures—Do We Save Lives? Mortality Rates Analysis Comparison in a Long-Term Follow-Up Cohort. Glob. Spine J. 2022;12:1443–1448. doi: 10.1177/2192568220982282. - DOI - PMC - PubMed
-
- Scura D., Piazza V.M. Spine Secrets Plus. Elsevier; Amsterdam, The Netherlands: 2021. Disability Evaluation.
-
- Jassal N.S. Treatment of Chronic Pain Conditions. Springer; Berlin/Heidelberg, Germany: 2017. Lumbar Spine History and Physical; pp. 33–35.
-
- Doğan M., Koçak M., Kılınç Ö.O., Ayvat F., Sütçü G., Ayvat E., Kılınç M., Ünver Ö., Yıldırım S.A. Functional range of motion in the upper extremity and trunk joints: Nine functional everyday tasks with inertial sensors. Gait Posture. 2019;70:141–147. doi: 10.1016/j.gaitpost.2019.02.024. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
