

Local Resection in Choroidal Melanoma: A Review
- PMID: 36498730
- PMCID: PMC9735844
- DOI: 10.3390/jcm11237156
Local Resection in Choroidal Melanoma: A Review
Abstract
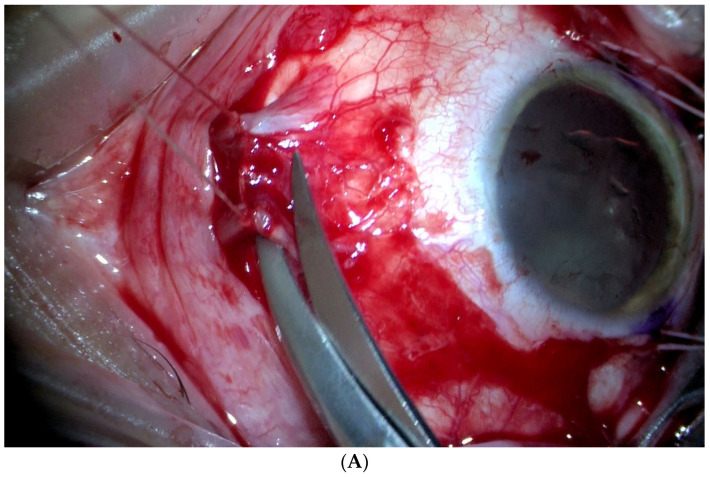
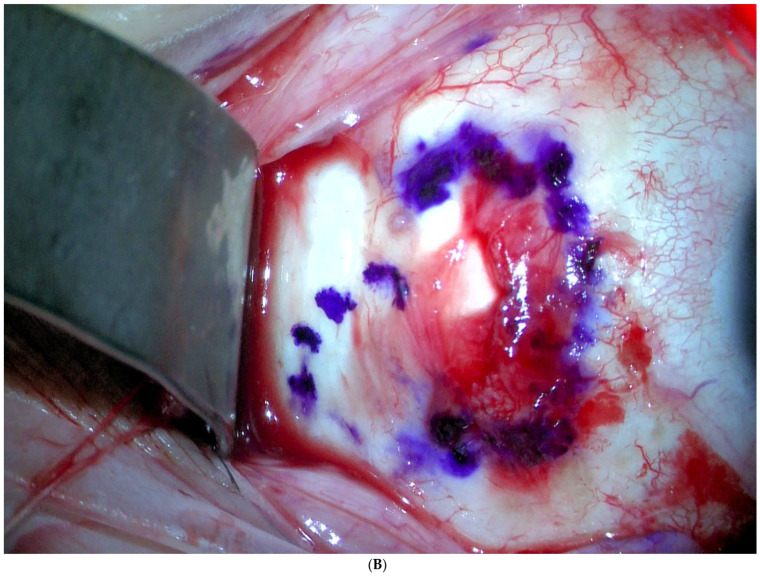
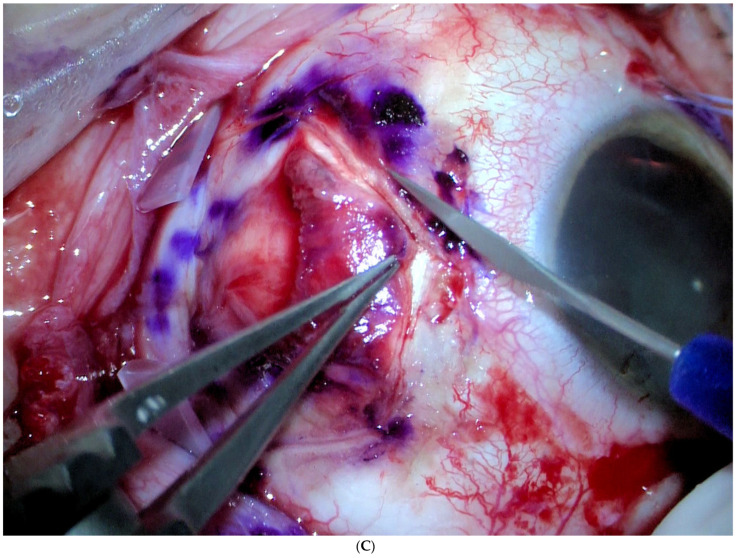
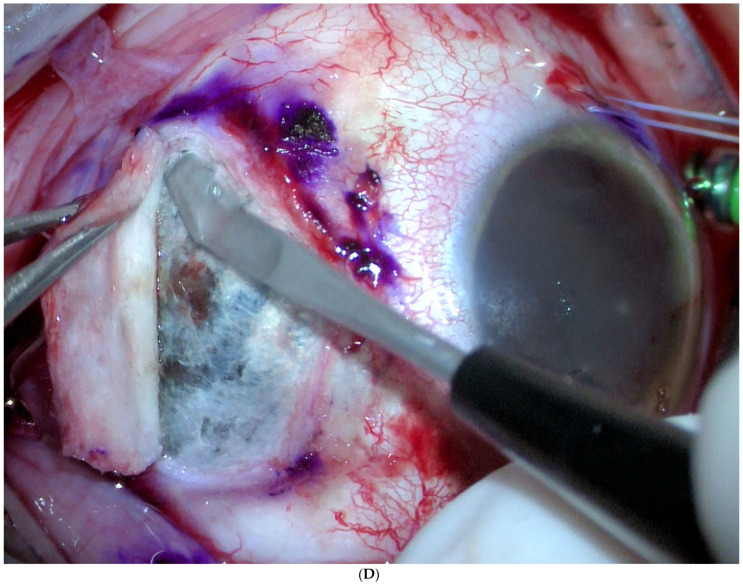
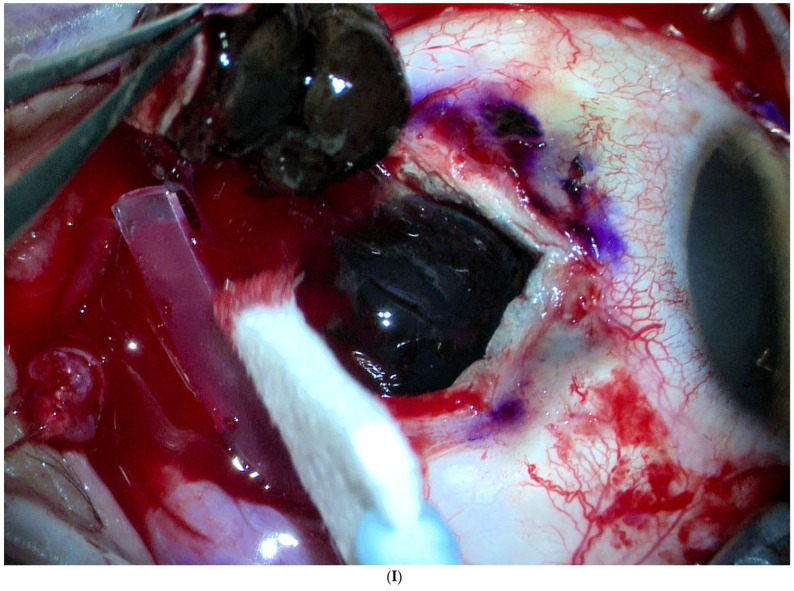
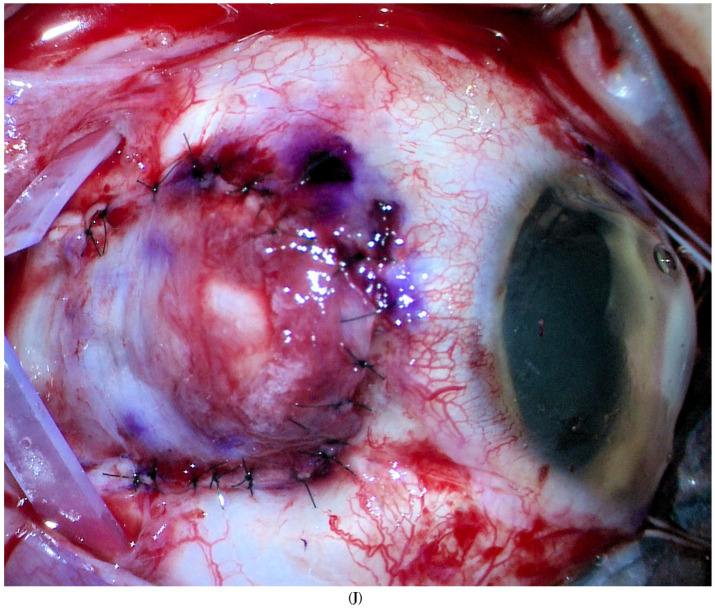
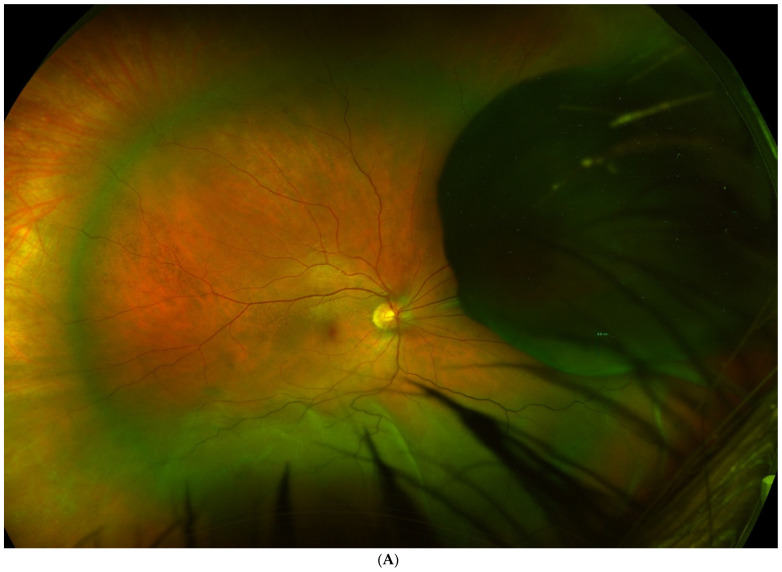
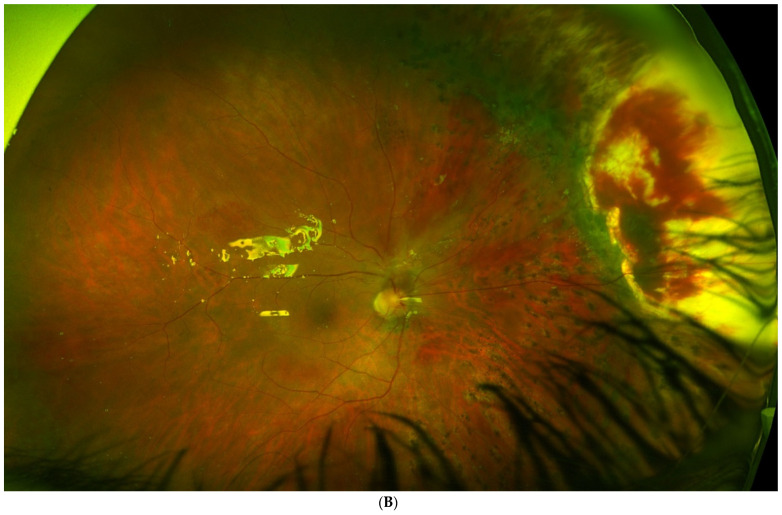
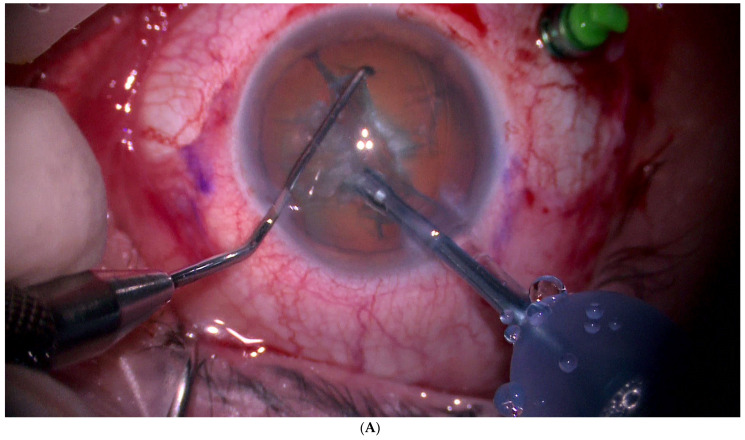
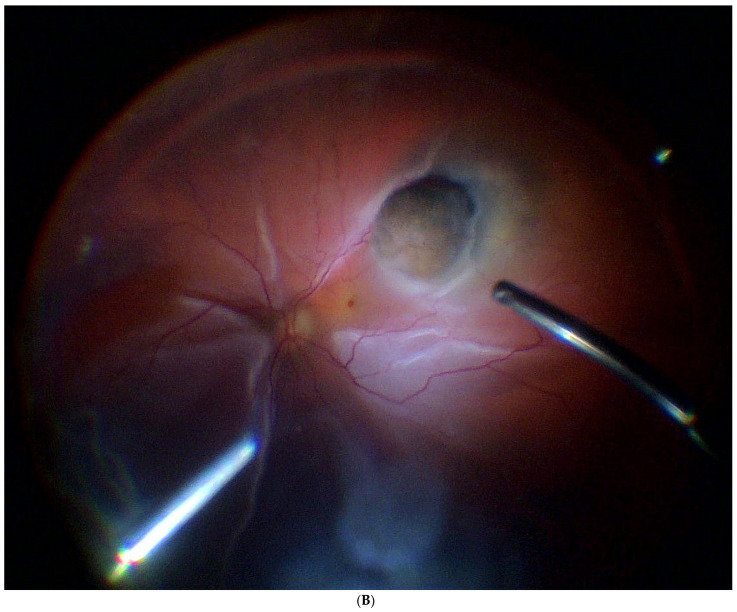
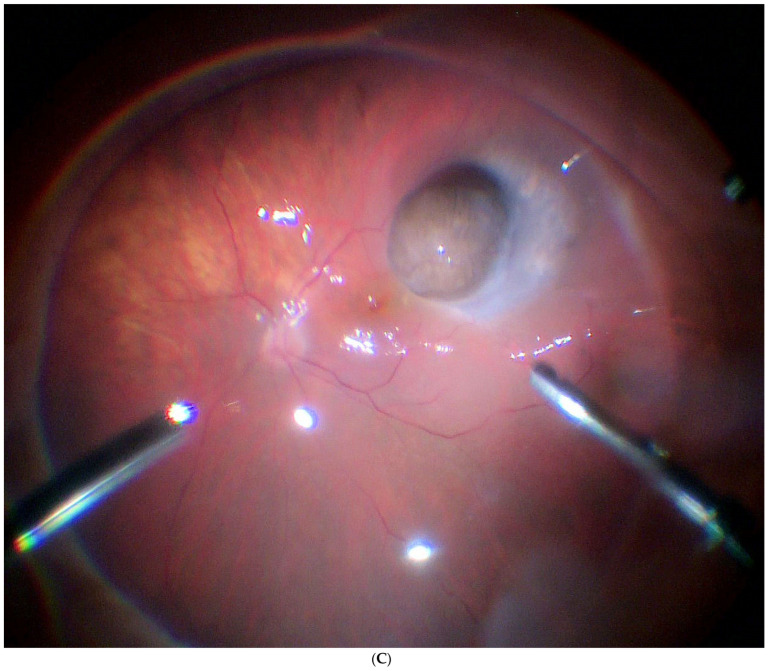
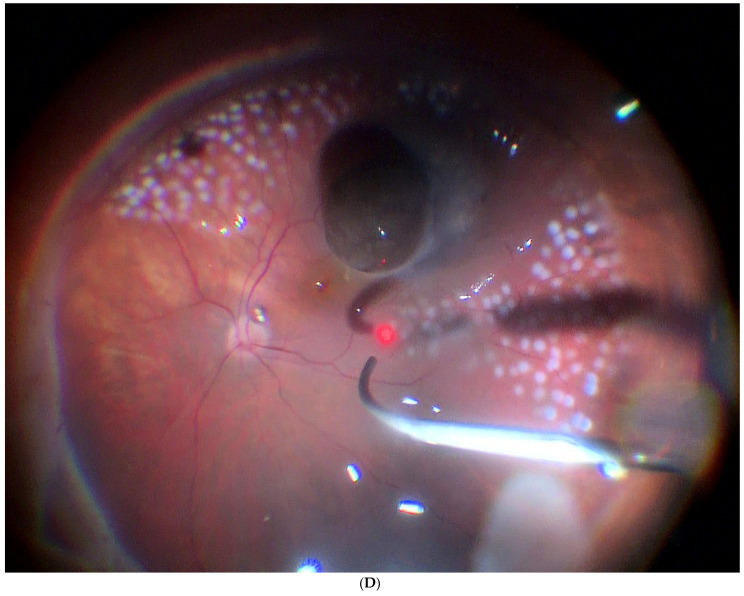
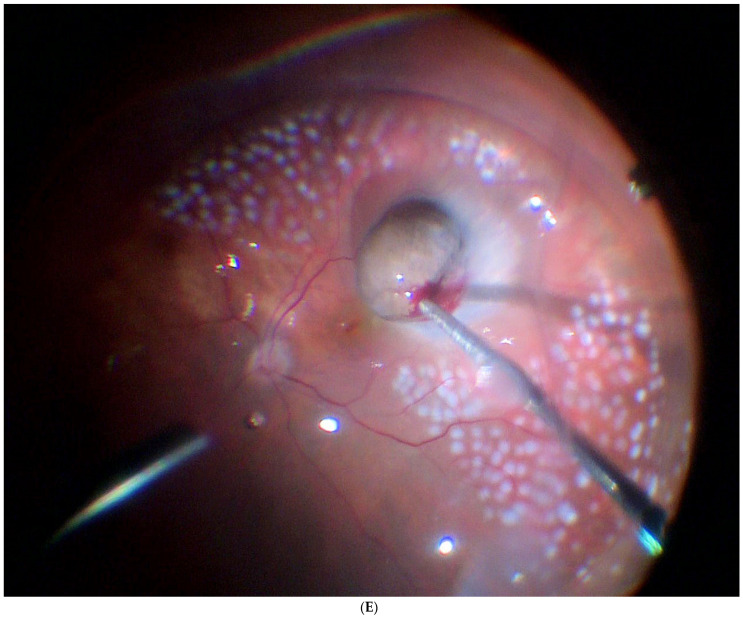
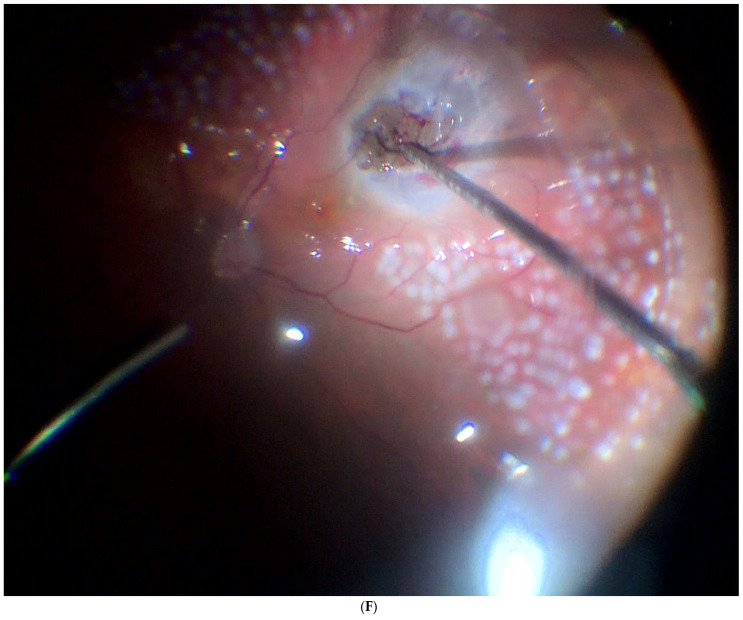
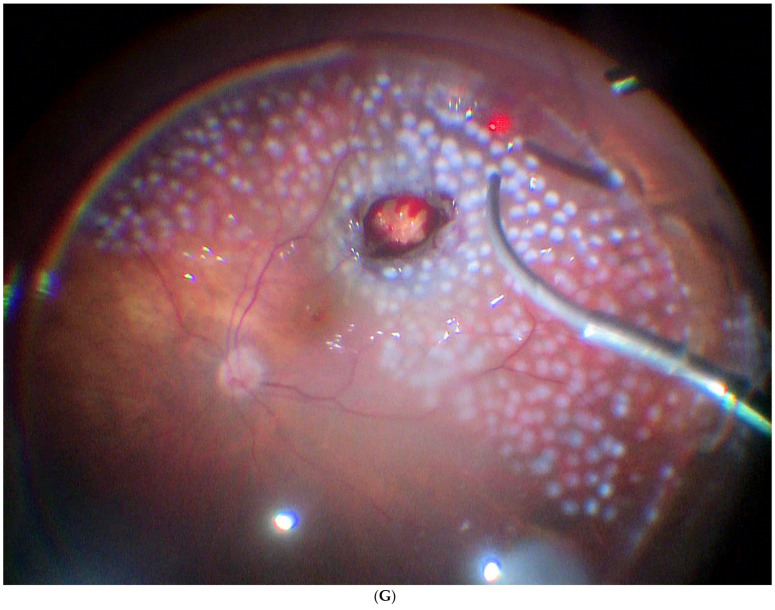
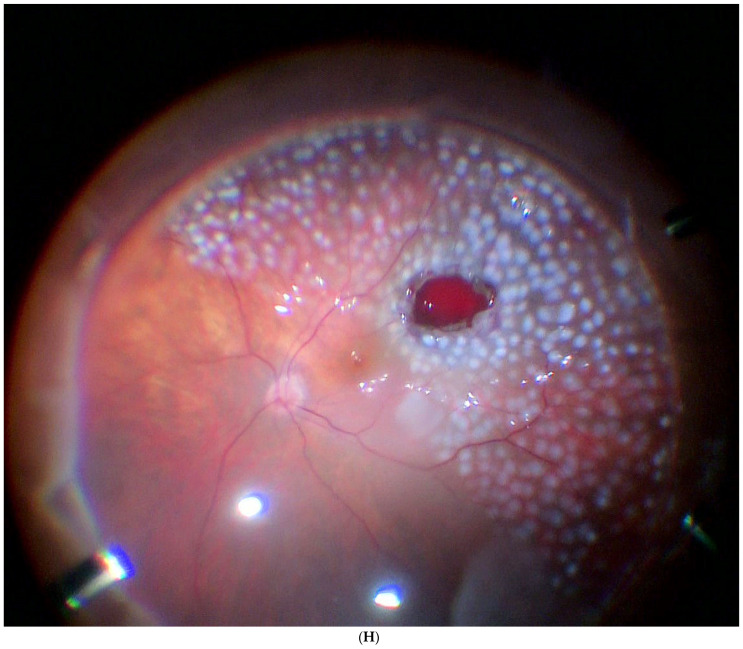
Surgical resection is widely used to treat small tumours located in the iris and the ciliary body, due to the accessibility of these sites. By contrast, surgical removal of choroidal tumours is substantially more challenging, which is why this procedure is performed only at specialised centres. In the present article, we review the literature on surgical resection of choroidal tumours, which can be performed as endoresection (ab interno) or transscleral resection (ab externo). An important aim of this review is to describe and compare the two approaches in terms of visual outcomes, survival rates, and complications. Both approaches are indicated for the removal of large tumours (thickness > 8 mm) with small base diameters. Surgical resection of the tumour allows clinicians to obtain valuable histopathologic and cytogenetic data from the specimen and eliminates the risks associated with radiotherapy. However, both of these surgical approaches are technically challenging procedures involving the risk of severe early and late postoperative complications.
Keywords: choroidectomy; exoresection; lamellar uveal melanoma resection; scleral resection; transscleral resection; uveal melanoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Damato B., Groenewald C. Clinical Ophthalmic Oncology. Elsevier Inc.; Amsterdam, The Netherlands: 2007. Uveal Malignant Melanoma: Management Options—Resection Techniques; pp. 259–266. - DOI
Publication types
LinkOut - more resources
Full Text Sources
