

Validity and Reliability of Wearable Motion Sensors for Clinical Assessment of Shoulder Function in Brachial Plexus Birth Injury
- PMID: 36502259
- PMCID: PMC9736020
- DOI: 10.3390/s22239557
Validity and Reliability of Wearable Motion Sensors for Clinical Assessment of Shoulder Function in Brachial Plexus Birth Injury
Abstract
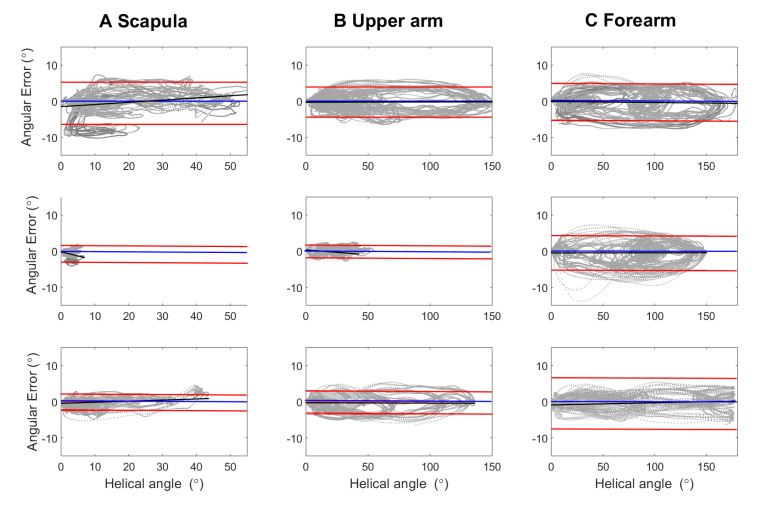
The modified Mallet scale (MMS) is commonly used to grade shoulder function in brachial plexus birth injury (BPBI) but has limited sensitivity and cannot grade scapulothoracic and glenohumeral mobility. This study aims to evaluate if the addition of a wearable inertial movement unit (IMU) system could improve clinical assessment based on MMS. The system validity was analyzed with simultaneous measurements with the IMU system and an optical camera system in three asymptomatic individuals. Test-retest and interrater reliability were analyzed in nine asymptomatic individuals and six BPBI patients. IMUs were placed on the upper arm, forearm, scapula, and thorax. Peak angles, range of motion, and average joint angular speed in the shoulder, scapulothoracic, glenohumeral, and elbow joints were analyzed during mobility assessments and MMS tasks. In the validity tests, clusters of reflective markers were placed on the sensors. The validity was high with an error standard deviation below 3.6°. Intraclass correlation coefficients showed that 90.3% of the 69 outcome scores showed good-to-excellent test-retest reliability, and 41% of the scores gave significant differences between BPBI patients and controls with good-to-excellent test-retest reliability. The interrater reliability was moderate to excellent, implying that standardization is important if the patient is followed-up longitudinally.
Keywords: brachial plexus birth injury; clinical evaluation; inertial movement unit; kinematic analysis; scapula movement; shoulder function.
Conflict of interest statement
The authors declare no conflict of interest. Fredrik Öhberg and Helena Grip are shareholders of the company AnyMo AB, which is manufacturing both sensors and analysis software used in this study.
Figures






Similar articles
-
Shoulder extension impairment with residual neonatal brachial plexus injury.J Shoulder Elbow Surg. 2023 Oct;32(10):2082-2088. doi: 10.1016/j.jse.2023.03.036. Epub 2023 May 11. J Shoulder Elbow Surg. 2023. PMID: 37178959
-
Scapulothoracic and glenohumeral contributions to motion in children with brachial plexus birth palsy.J Shoulder Elbow Surg. 2014 Mar;23(3):327-38. doi: 10.1016/j.jse.2013.06.023. Epub 2013 Sep 24. J Shoulder Elbow Surg. 2014. PMID: 24075782
-
Effect of Glenohumeral Reduction Type Combined With Tendon Transfer for Brachial Plexus Injury on Objective, Functional, and Patient-Reported Outcomes.J Hand Surg Am. 2021 Jul;46(7):624.e1-624.e11. doi: 10.1016/j.jhsa.2020.11.021. Epub 2021 Jan 30. J Hand Surg Am. 2021. PMID: 33526294
-
Perspectives on glenohumeral joint contractures and shoulder dysfunction in children with perinatal brachial plexus palsy.J Hand Ther. 2015 Apr-Jun;28(2):176-83; quiz 184. doi: 10.1016/j.jht.2014.12.001. Epub 2014 Dec 18. J Hand Ther. 2015. PMID: 25835253 Review.
-
Evaluation and management of brachial plexus birth palsy.Orthop Clin North Am. 2014 Apr;45(2):225-32. doi: 10.1016/j.ocl.2013.12.004. Epub 2014 Jan 29. Orthop Clin North Am. 2014. PMID: 24684916 Review.
Cited by
-
Monitoring Scapular Kinematics through Wearable Magneto-Inertial Measurement Units: State of the Art and New Frontiers.Sensors (Basel). 2023 Aug 4;23(15):6940. doi: 10.3390/s23156940. Sensors (Basel). 2023. PMID: 37571723 Free PMC article.
-
Automated Assessment of Upper Extremity Function with the Modified Mallet Score Using Single-Plane Smartphone Videos.Sensors (Basel). 2025 Mar 6;25(5):1619. doi: 10.3390/s25051619. Sensors (Basel). 2025. PMID: 40096483 Free PMC article.
References
-
- Van der Looven R., Le Roy L., Tanghe E., Samijn B., Roets E., Pauwels N., Deschepper E., De Muynck M., Vingerhoets G., Van den Broeck C. Risk factors for neonatal brachial plexus palsy: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2020;62:673–683. doi: 10.1111/dmcn.14381. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
