

Numerical analysis of the effects of padded pelvic belts as a treatment for sacroiliac joint dysfunction
- PMID: 36502302
- PMCID: PMC10357188
- DOI: 10.3233/BME-221490
Numerical analysis of the effects of padded pelvic belts as a treatment for sacroiliac joint dysfunction
Abstract
Background: Pain related to the sacroiliac joint (SIJ) accounts for low back pain in 15%-30% of patients. One of the most common treatment options is the use of pelvic belts. Various types of pelvic belts exist; however, the mechanisms underlying treatment and their effectiveness remain unclear to date.
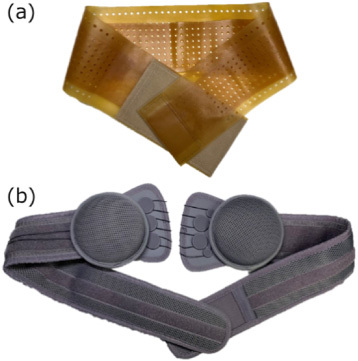
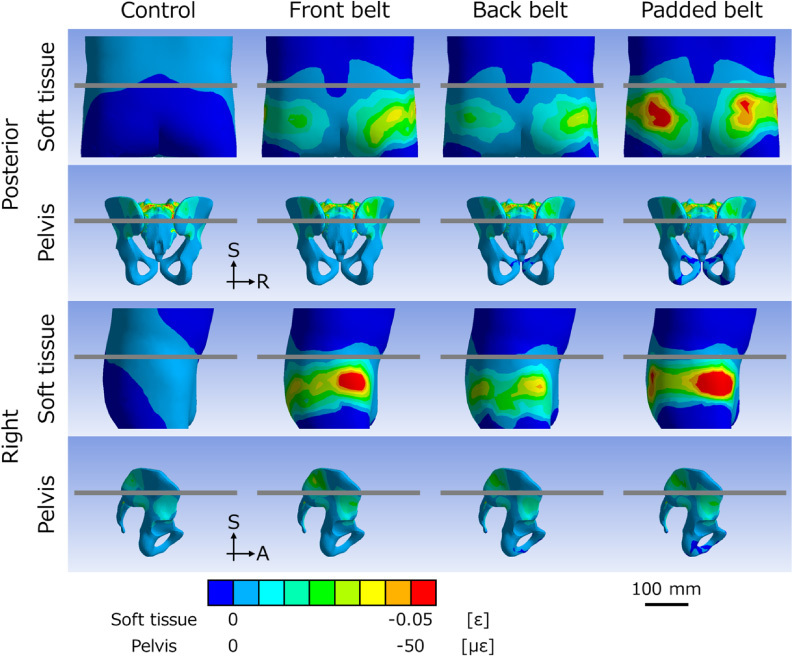
Objective: To analyze stress distribution in the pelvis when a pelvic rubber belt or a padded pelvic belt is applied, to assess the effectiveness of treatment from a numerical biomechanical perspective.
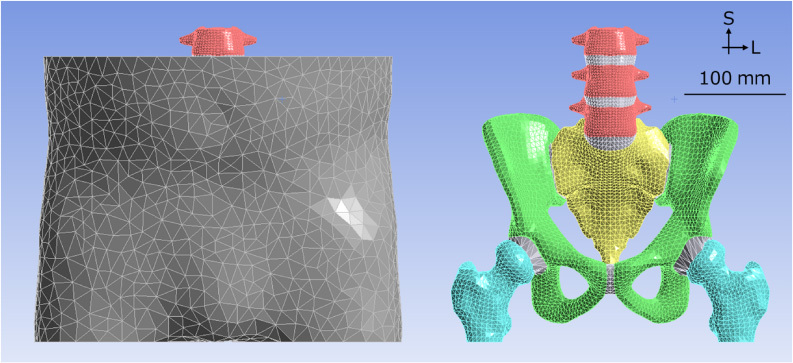
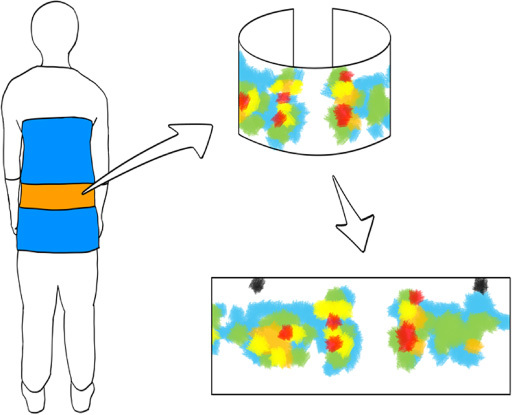
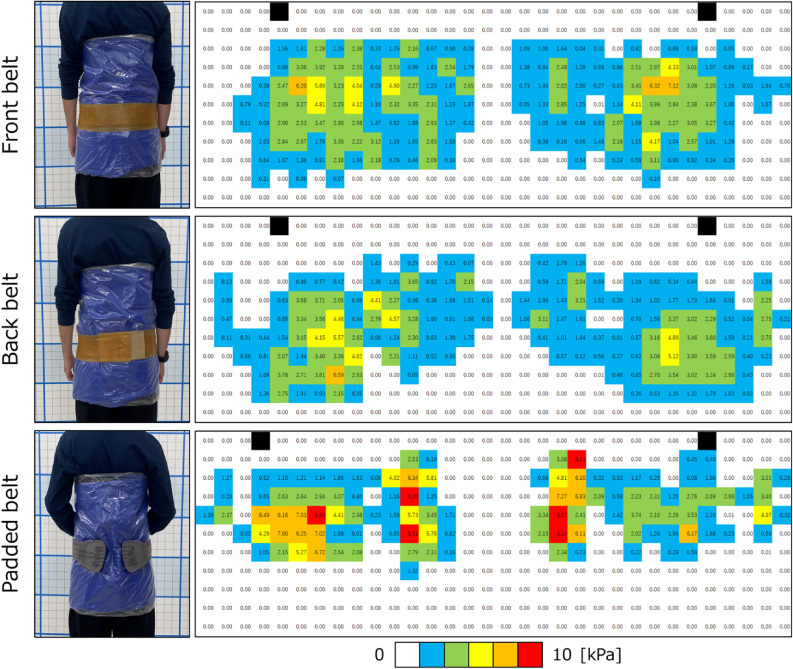
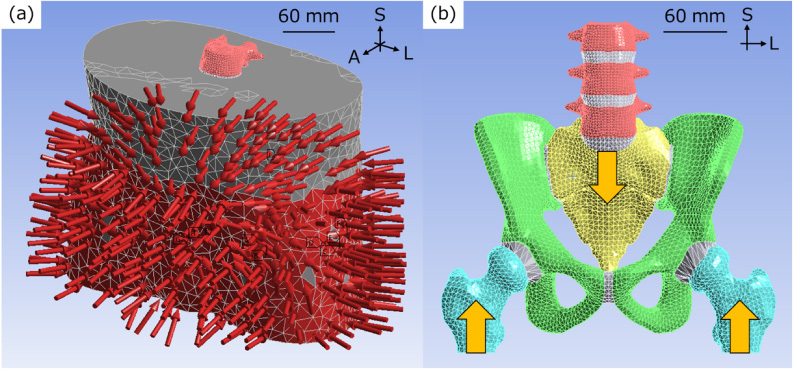
Methods: The pressure distribution at the pelvic belts was measured using a device and subsequently modeled with the finite element method of a pelvis with soft tissues. The stress environment when wearing a pelvic belt in a double-leg stance was simulated.
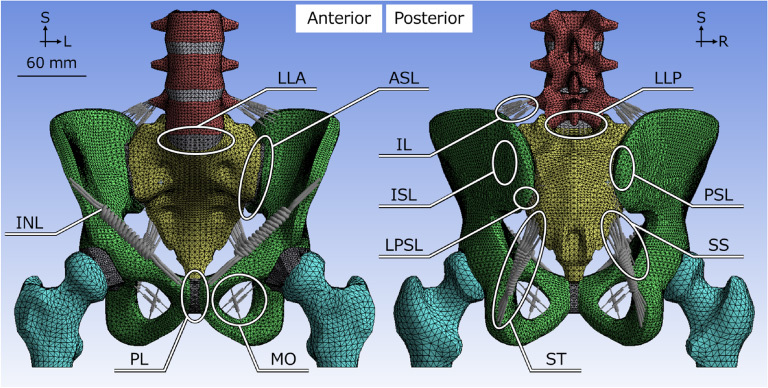
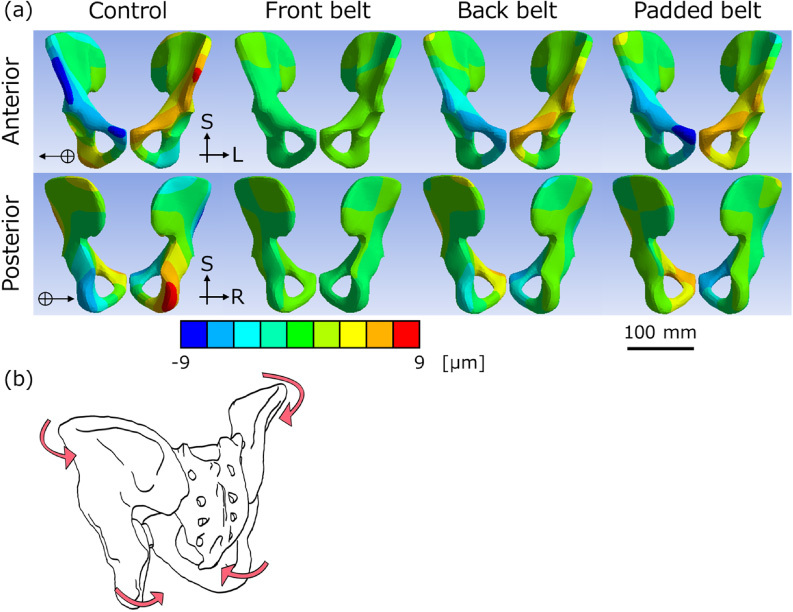
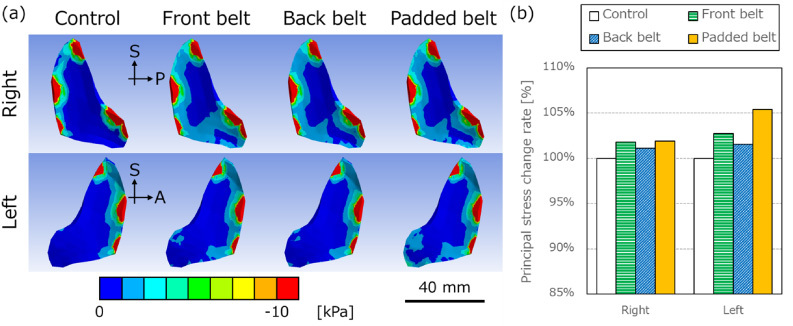
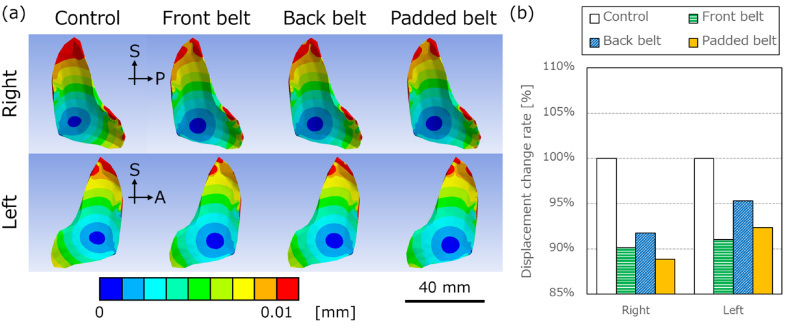
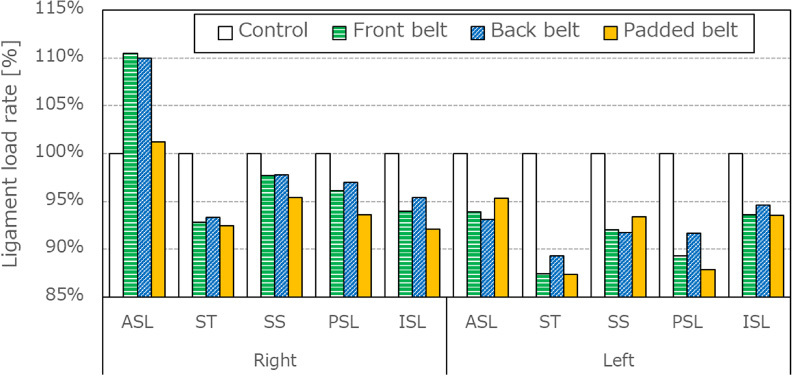
Results: With the application of pelvic belts, the innominate bone rotated outward, which was termed an out-flare. This caused the SIJ to compress and cause reduction in sacrotuberous, sacrospinous, interosseous, and posterior sacroiliac ligament loading. Padded pelvic belts decreased the SIJ displacement to a greater extent than in pelvic rubber belts.
Conclusion: Pelvic belts aid in compressing the SIJ and reduce its mobility.
Keywords: Finite element analysis; low back pain; numerical analysis; pelvic belt; sacroiliac joint dysfunction.
Conflict of interest statement
None to report.
Figures
Similar articles
-
Pelvic belt effects on sacroiliac joint ligaments: a computational approach to understand therapeutic effects of pelvic belts.Pain Physician. 2014 Jan-Feb;17(1):43-51. Pain Physician. 2014. PMID: 24452644
-
Pelvic belt effects on pelvic morphometry, muscle activity and body balance in patients with sacroiliac joint dysfunction.PLoS One. 2015 Mar 17;10(3):e0116739. doi: 10.1371/journal.pone.0116739. eCollection 2015. PLoS One. 2015. PMID: 25781325 Free PMC article. Clinical Trial.
-
Pelvic Belt Effects on Health Outcomes and Functional Parameters of Patients with Sacroiliac Joint Pain.PLoS One. 2015 Aug 25;10(8):e0136375. doi: 10.1371/journal.pone.0136375. eCollection 2015. PLoS One. 2015. PMID: 26305790 Free PMC article. Clinical Trial.
-
In-silico pelvis and sacroiliac joint motion-A review on published research using numerical analyses.Clin Biomech (Bristol). 2019 Jan;61:95-104. doi: 10.1016/j.clinbiomech.2018.12.005. Epub 2018 Dec 6. Clin Biomech (Bristol). 2019. PMID: 30544056
-
Movement of the sacroiliac joint: Anatomy, systematic review, and biomechanical considerations.Proc Inst Mech Eng H. 2021 Mar;235(3):357-364. doi: 10.1177/0954411920978021. Epub 2020 Nov 30. Proc Inst Mech Eng H. 2021. PMID: 33256545
References
-
- Bernard T.N. and Kirkaldy-Wills W.H., Recognizing specific characteristics of nonspecific low back pain, Clin Orthop Relat Res 217 (1987), 266–280. - PubMed
-
- Schwarzer A.C., Aprill C.N. and Bogduk N., The sacroiliac joint in chronic low back pain, Spine 20(1) (1995), 31–37. - PubMed
-
- Forst S.L., Wheeler M.T., Fortin J.D. and Vilensky J.A., The sacroiliac joint: Anatomy, physiology and clinical significance, Pain Physician 9(1) (2006), 61–67. - PubMed
-
- Lovejoy C.O., Evolution of the human lumbopelvic region and its relationship to some clinical deficits of the spine and pelvis, in: Movement, Stability and Lumbopelvic Pain: Integration of Research and Therapy, Vleeming A., Mooney V. and Stoeckart R. (eds), Churchill Livingstone, London, 2007, pp. 141–158.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
