

Performance of spiral UTE-MRI of the lung in post-COVID patients
- PMID: 36503014
- PMCID: PMC9731813
- DOI: 10.1016/j.mri.2022.12.002
Performance of spiral UTE-MRI of the lung in post-COVID patients
Abstract
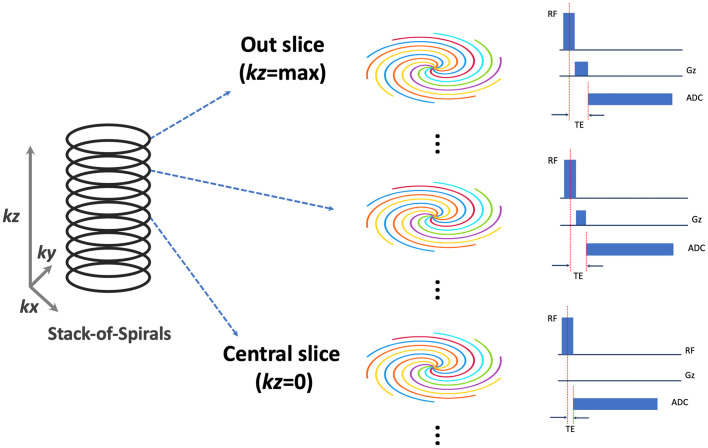
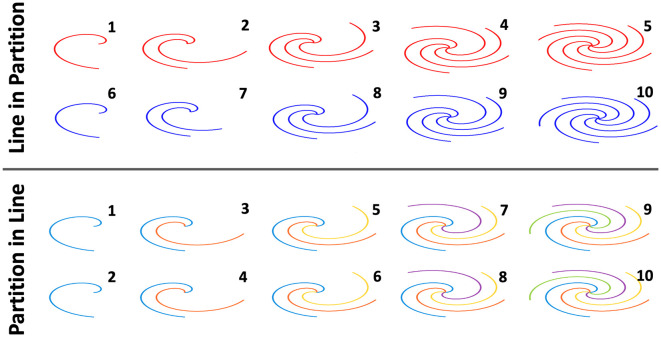
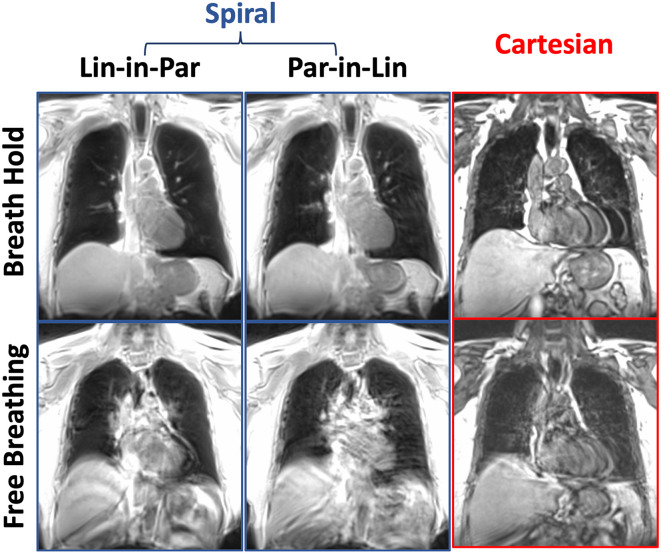
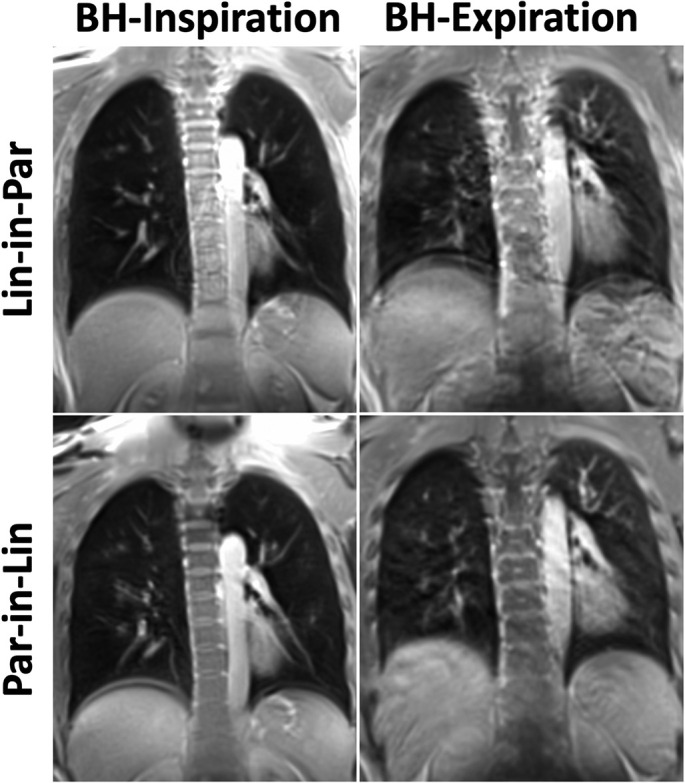
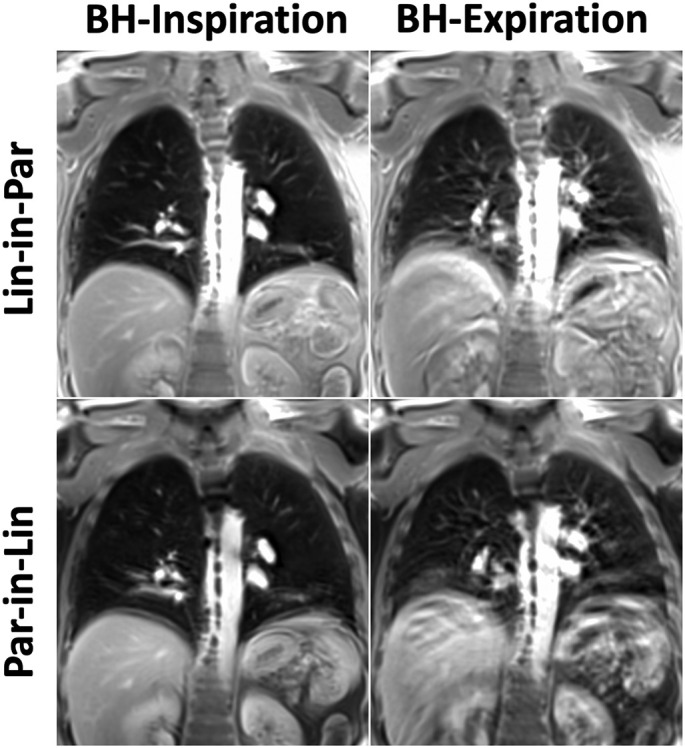
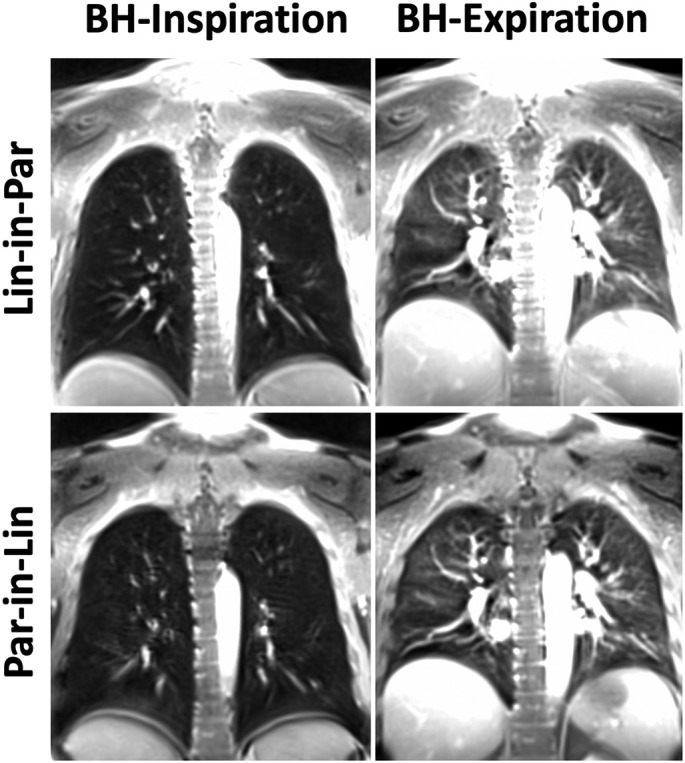
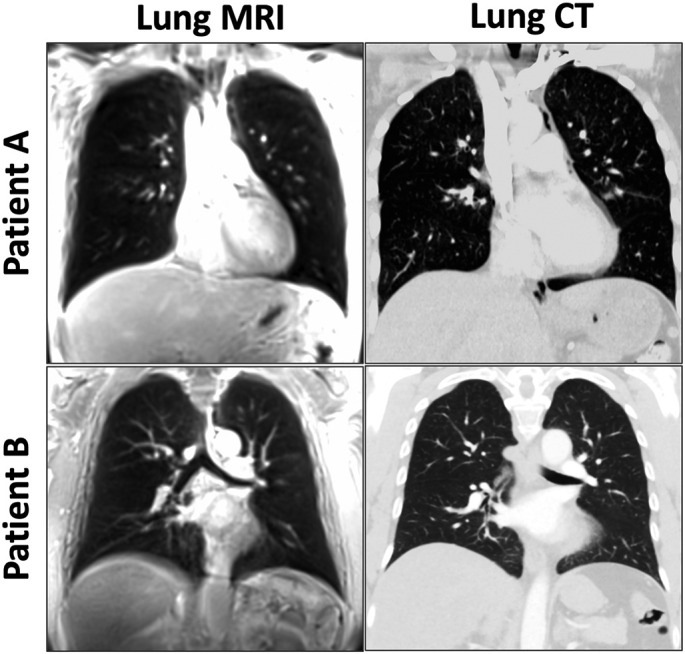
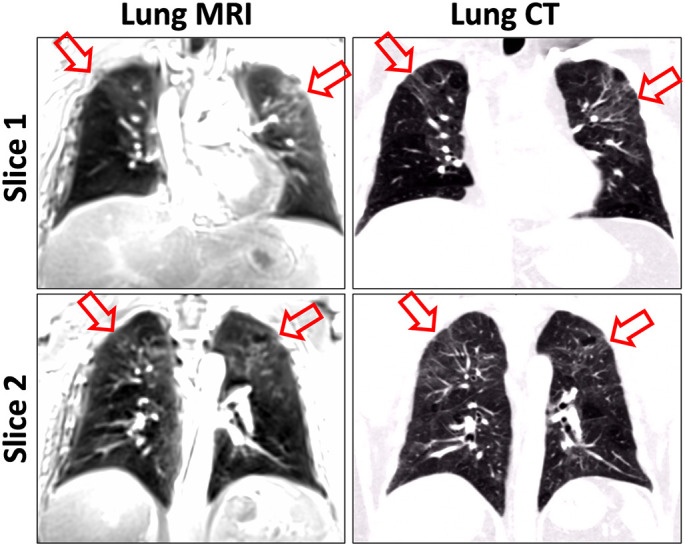
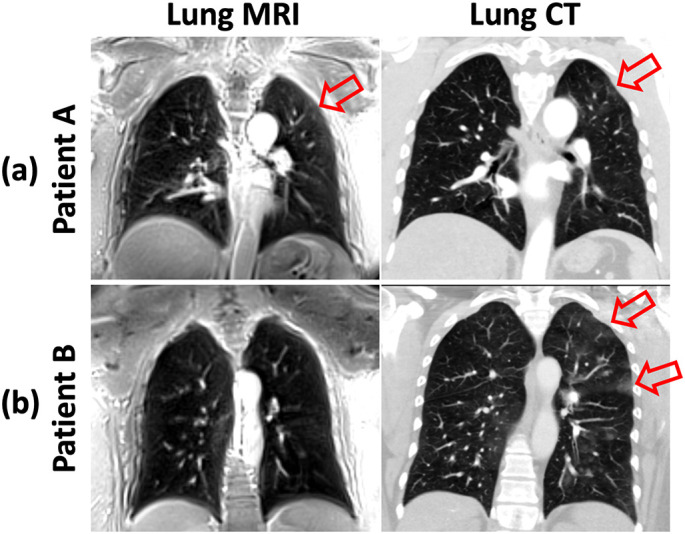
Patients recovered from COVID-19 may develop long-COVID symptoms in the lung. For this patient population (post-COVID patients), they may benefit from longitudinal, radiation-free lung MRI exams for monitoring lung lesion development and progression. The purpose of this study was to investigate the performance of a spiral ultrashort echo time MRI sequence (Spiral-VIBE-UTE) in a cohort of post-COVID patients in comparison with CT and to compare image quality obtained using different spiral MRI acquisition protocols. Lung MRI was performed in 36 post-COVID patients with different acquisition protocols, including different spiral sampling reordering schemes (line in partition or partition in line) and different breath-hold positions (inspiration or expiration). Three experienced chest radiologists independently scored all the MR images for different pulmonary structures. Lung MR images from spiral acquisition protocol that received the highest image quality scores were also compared against corresponding CT images in 27 patients for evaluating diagnostic image quality and lesion identification. Spiral-VIBE-UTE MRI acquired with the line in partition reordering scheme in an inspiratory breath-holding position achieved the highest image quality scores (score range = 2.17-3.69) compared to others (score range = 1.7-3.29). Compared to corresponding chest CT images, three readers found that 81.5% (22 out of 27), 81.5% (22 out of 27) and 37% (10 out of 27) of the MR images were useful, respectively. Meanwhile, they all agreed that MRI could identify significant lesions in the lungs. The Spiral-VIBE-UTE sequence allows for fast imaging of the lung in a single breath hold. It could be a valuable tool for lung imaging without radiation and could provide great value for managing different lung diseases including assessment of post-COVID lesions.
Keywords: COVID-19; Lung imaging; MRI; Post-COVID; Spiral sampling; Stack-of-spirals; Ultrashort echo time.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Feasibility of chest spiral 3D ultrashort echo time magnetic resonance imaging for intrathoracic metastasis work-up in breast cancer.J Thorac Dis. 2023 Oct 31;15(10):5485-5493. doi: 10.21037/jtd-23-1006. Epub 2023 Sep 25. J Thorac Dis. 2023. PMID: 37969267 Free PMC article.
-
Comparison of diagnostic performance for pulmonary nodule detection between free-breathing spiral ultrashort echo time and free-breathing radial volumetric interpolated breath-hold examination.BMC Med Imaging. 2025 Jan 10;25(1):15. doi: 10.1186/s12880-024-01536-6. BMC Med Imaging. 2025. PMID: 39794718 Free PMC article.
-
Detection of lung lesions in breath-hold VIBE and free-breathing Spiral VIBE MRI compared to CT.Insights Imaging. 2021 Nov 24;12(1):175. doi: 10.1186/s13244-021-01124-0. Insights Imaging. 2021. PMID: 34817715 Free PMC article.
-
Outracing Lung Signal Decay - Potential of Ultrashort Echo Time MRI.Rofo. 2019 May;191(5):415-423. doi: 10.1055/a-0715-2246. Epub 2018 Sep 26. Rofo. 2019. PMID: 30257269 English.
-
Echocardiography and Lung Ultrasound in Long COVID and Post-COVID Syndrome, a Review Document of the Austrian Society of Pneumology and the Austrian Society of Ultrasound in Medicine.J Ultrasound Med. 2023 Feb;42(2):269-277. doi: 10.1002/jum.16068. Epub 2022 Jul 30. J Ultrasound Med. 2023. PMID: 35906952 Free PMC article. Review.
Cited by
-
Discovery Viewer (DV): Web-Based Medical AI Model Development Platform and Deployment Hub.Bioengineering (Basel). 2023 Dec 6;10(12):1396. doi: 10.3390/bioengineering10121396. Bioengineering (Basel). 2023. PMID: 38135987 Free PMC article.
-
The Role of Proton MRI to Evaluate Patient Pathophysiology in Severe Asthma.Radiol Cardiothorac Imaging. 2023 Dec;5(6):e230372. doi: 10.1148/ryct.230372. Radiol Cardiothorac Imaging. 2023. PMID: 38166342 Free PMC article. No abstract available.
-
Lung T2 * mapping using 3D ultrashort TE with tight intervals δTE.Magn Reson Med. 2023 Nov;90(5):2001-2010. doi: 10.1002/mrm.29756. Epub 2023 Jun 8. Magn Reson Med. 2023. PMID: 37288577 Free PMC article.
-
Single breath-hold volumetric lung imaging at 0.55T using stack-of-spiral (SoS) out-in balanced SSFP.Magn Reson Med. 2025 May;93(5):1999-2007. doi: 10.1002/mrm.30386. Epub 2024 Nov 28. Magn Reson Med. 2025. PMID: 39607896 Free PMC article.
-
Changes of in vivo electrical conductivity in the brain and torso related to age, fat fraction and sex using MRI.Sci Rep. 2024 Jul 12;14(1):16109. doi: 10.1038/s41598-024-67014-9. Sci Rep. 2024. PMID: 38997324 Free PMC article.
References
-
- COVID-19 Map - Johns Hopkins Coronavirus Resource Center 2022. https://coronavirus.jhu.edu/map.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
