

Hematologic and inflammatory parameters for determining severity of odontogenic infections at admission: a retrospective study
- PMID: 36503406
- PMCID: PMC9743669
- DOI: 10.1186/s12879-022-07934-x
Hematologic and inflammatory parameters for determining severity of odontogenic infections at admission: a retrospective study
Abstract
Background: Severe odontogenic infections in the head and neck region, especially necrotizing soft tissue infection (NSTI) and deep neck abscess, are potentially fatal due to their delayed diagnosis and treatment. Clinically, it is often difficult to distinguish NSTI and deep neck abscess in its early stage from cellulitis, and the decision to perform contrast-enhanced computed tomography imaging for detection is often a challenge. This retrospective case-control study aimed to examine the utility of routine blood tests as an adjunctive diagnostic tool for NSTI in the head and neck region and deep neck abscesses.
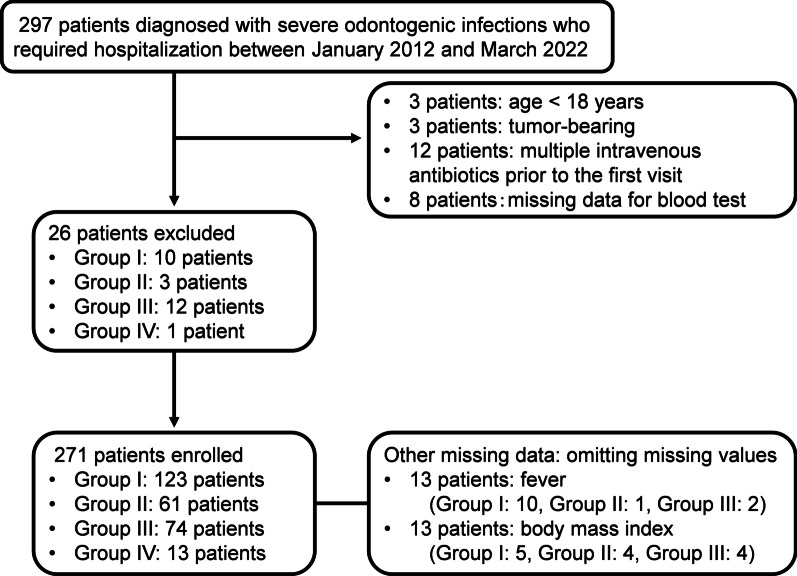
Methods: Patients with severe odontogenic infections in the head and neck region that required hospitalization were classified into four groups. At admission, hematologic and inflammatory parameters were calculated according to the blood test results. In addition, a decision tree analysis was performed to detect NSTI and deep neck abscesses.
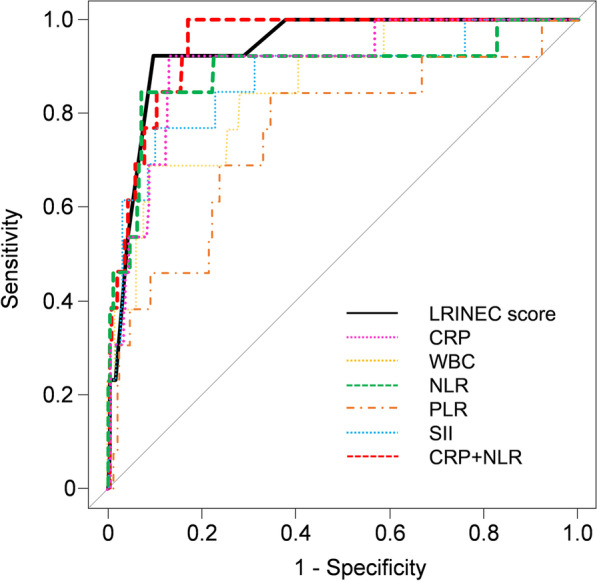
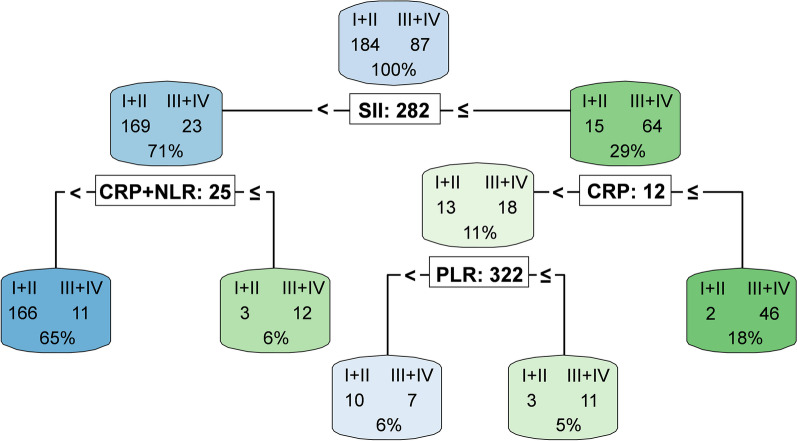
Results: There were 271 patients, 45.4% in Group I (cellulitis), 22.5% in Group II (cellulitis with shallow abscess formation), 27.3% in Group III (deep neck abscess), and 4.8% in Group IV (NSTI). All hematologic and inflammatory parameters were higher in Groups III and IV. The Laboratory Risk Indicator for Necrotizing Fasciitis score, with a cut-off value of 6 and C-reactive protein (CRP) + the neutrophil-to-lymphocyte ratio (NLR), with a cut-off of 27, were remarkably useful for the exclusion diagnosis for Group IV. The decision tree analysis showed that the systemic immune-inflammation index (SII) of ≥ 282 or < 282 but with a CRP + NLR of ≥ 25 suggests Group III + IV and the classification accuracy was 89.3%.
Conclusions: Hematologic and inflammatory parameters calculated using routine blood tests can be helpful as an adjunctive diagnostic tool in the early diagnosis of potentially fatal odontogenic infections. An SII of ≥ 282 or < 282 but with a CRP + NLR of ≥ 25 can be useful in the decision-making for performing contrast-enhanced computed tomography imaging.
Keywords: Cellulitis; Contrast-enhanced computed tomography; Deep neck abscess; Necrotizing soft tissue infection; Neutrophil-to-lymphocyte ratio; Systemic immune-inflammation index.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cervical Necrotizing Fasciitis, Diagnosis and Treatment of a Rare Life-Threatening Infection.Ear Nose Throat J. 2023 Mar;102(3):NP109-NP113. doi: 10.1177/0145561321991341. Epub 2021 Feb 11. Ear Nose Throat J. 2023. PMID: 33570428
-
The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections.Crit Care Med. 2004 Jul;32(7):1535-41. doi: 10.1097/01.ccm.0000129486.35458.7d. Crit Care Med. 2004. PMID: 15241098
-
The Role of Neutrophil-to-Lymphocyte Ratio and Mean Platelet Volume in Diagnosing Odontogenic and Non-odontogenic Head and Neck Abscesses.Cureus. 2024 Oct 30;16(10):e72711. doi: 10.7759/cureus.72711. eCollection 2024 Oct. Cureus. 2024. PMID: 39618643 Free PMC article.
-
Skin and soft tissue infections.Prim Care. 2006 Sep;33(3):697-710. doi: 10.1016/j.pop.2006.06.005. Prim Care. 2006. PMID: 17088156 Review.
-
Necrotizing Soft Tissue Infections (NSTI): Pearls and Pitfalls for the Emergency Clinician.J Emerg Med. 2022 Apr;62(4):480-491. doi: 10.1016/j.jemermed.2021.12.012. Epub 2022 Jan 31. J Emerg Med. 2022. PMID: 35115188 Review.
Cited by
-
Comparative Characterization of Procalcitonin (Sensitivity, Specificity, Predictability, and Cut-Off Reference Values) as a Marker of Inflammation in Odontogenic Abscesses of the Head and Neck in the Female Population.Cureus. 2023 Nov 3;15(11):e48207. doi: 10.7759/cureus.48207. eCollection 2023 Nov. Cureus. 2023. PMID: 38050495 Free PMC article.
-
Predictive value of platelet count-related ratios for severity in biliary Escherichia coli and Klebsiella pneumonia bloodstream infections.Eur J Clin Microbiol Infect Dis. 2025 Jul;44(7):1597-1604. doi: 10.1007/s10096-025-05120-w. Epub 2025 Apr 11. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40214861
-
Impact of Treatment on Systemic Immune-Inflammatory Index and Other Inflammatory Markers in Odontogenic Cervicofacial Phlegmon Cases: A Retrospective Study.Biomedicines. 2023 Jun 14;11(6):1710. doi: 10.3390/biomedicines11061710. Biomedicines. 2023. PMID: 37371805 Free PMC article.
-
The Role of qSOFA, Derived Neutrophil-to-Lymphocyte Ratio, MEWS, and PIRO Scores in Predicting the Severity of Odontogenic Infections in Young and Adult Patients.Biomedicines. 2025 Feb 20;13(3):532. doi: 10.3390/biomedicines13030532. Biomedicines. 2025. PMID: 40149510 Free PMC article.
-
Treatment Behaviors of Patients With Odontogenic Infections During the COVID-19 Pandemic.Cureus. 2025 Mar 29;17(3):e81414. doi: 10.7759/cureus.81414. eCollection 2025 Mar. Cureus. 2025. PMID: 40296983 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
