

Severe COVID-19-associated myocarditis with cardiogenic shock - management with assist devices - a case report & review
- PMID: 36503438
- PMCID: PMC9742039
- DOI: 10.1186/s12871-022-01890-4
Severe COVID-19-associated myocarditis with cardiogenic shock - management with assist devices - a case report & review
Abstract
Background: Primary viral myocarditis associated with severe acute respiratory syndrome coronavirus 2 (SARS-Cov2) infection is a rare diagnosis.
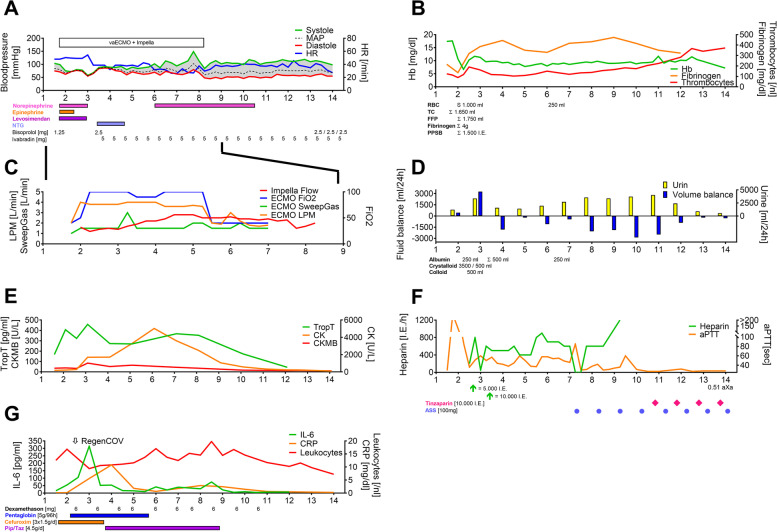
Case presentation: We report the case of an unvaccinated, healthy patient with cardiogenic shock in the context of a COVID-19-associated myocarditis and therapy with simultaneous veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and percutaneous left ventricular decompression therapy with an Impella. The aim of this review is to provide an overview of therapeutic options for patients with COVID-19-associated myocarditis.
Conclusions: The majority of patients required a combination of two assist devices to achieve sufficient cardiac output until recovery of left ventricular ejection fraction. Due to the rapid onset of this fulminant cardiogenic shock immediate invasive bridging therapy in a specialized center was lifesaving.
Keywords: Critical care; Extracorporeal membrane oxygenation; Heart failure; Impella; Myocarditis; SARS-COV-2.
© 2022. The Author(s).
Conflict of interest statement
ANF received speaker fees from P.J. Dahlhausen & Co. GmbH, Colone, Germany and received the Sedana Medical Research Grant 2020. FJR received speaker fees from Helios Germany, university hospital Würzburg and Keller Medical GmbH. FJR received financial support by HemoSonics LLC, pharma-consult Petersohn and Boehringer Ingelheim. KZ has received honoraria for participation in advisory board meetings for Haemonetics and Vifor and received speaker fees from CSL Behring and GE Healthcare. He is the Principal Investigator of the EU-Horizon 2020 project ENVISION (Intelligent plug-and-play digital tool for real-time surveillance of COVID-19 patients and smart decision-making in Intensive Care Units) and Horizon Europe 2021 project COVend (Biomarker and AI-supported FX06 therapy to prevent progression from mild and moderate to severe stages of COVID-19). SN, SF and MS stated that they had no interests which might be perceived as posing a conflict or bias.
Figures
References
-
- Guarracino F, Vetrugno L, Forfori F, Corradi F, Orso D, Bertini P, Ortalda A, Federici N, Copetti R, Bove T. Lung, heart, vascular, and diaphragm ultrasound examination of COVID-19 patients: a comprehensive approach. J Cardiothorac Vasc Anesth. 2021;35(6):1866–1874. doi: 10.1053/j.jvca.2020.06.013. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
