

Prognostic value of elastic lamina staining in patients with stage III colon cancer
- PMID: 36503509
- PMCID: PMC9743714
- DOI: 10.1186/s12957-022-02865-y
Prognostic value of elastic lamina staining in patients with stage III colon cancer
Abstract
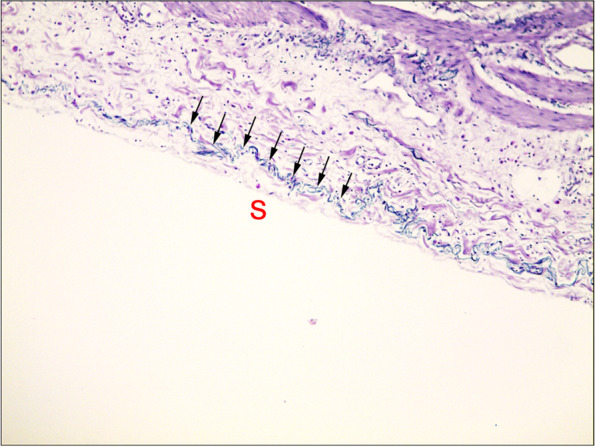
Objective: The objectives of this study were to analyze the difference between the preoperative radiological and postoperative pathological stages of colorectal cancer (CRC) and explore the feasibility of elastic lamina invasion (ELI) as a prognostic marker for patients with stage III colon cancer.
Methods: A total of 105 consecutive patients underwent radical surgery (R0 resection) for stage III colon cancer at the Cancer Hospital of China Medical University between January 2015 and December 2017. Clinicopathological features, including radiological stage and elastic lamina staining, were analyzed for prognostic significance in stage III colon cancer.
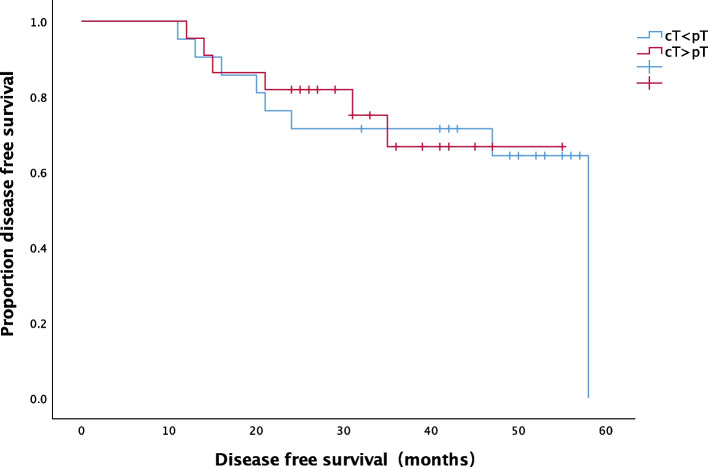
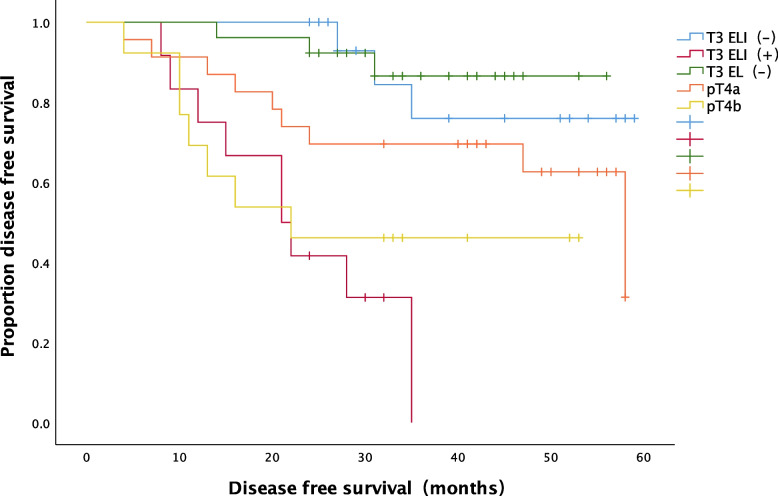
Results: A total of 105 patients with stage III colon cancer who met the criteria and had complete data available were included. The median follow-up period of survivors was 41 months. During the follow-up period, 33 (31.4%) patients experienced recurrence after radical resection, and the 3-year disease-free survival (DFS) rate was 64.8%. The consistency between preoperative radiological and postoperative pathological staging was poor (κ = 0.232, P < 0.001). The accuracy of ≤ T2 stage diagnoses was 97.1% (102/105), that of T3 stage was 60.9% (64/105), that of T4a stage was 68.6% (72/105) and that of T4b stage was 91.4% (96/105). The DFS rate of T3 ELI (+) patients was significantly lower than that of both T3 ELI (-) patients (P = 0.000) and pT4a patients (P = 0.013). The DFS rate of T3 ELI (-) patients was significantly higher than that of pT4b patients (P=0.018). T3 ELI (+) (HR (Hazard ratio), 8.444 [95% CI, 1.736-41.067]; P = 0.008), T4b (HR, 57.727[95% CI, 5.547-600.754]; P = 0.001), N2 stage (HR, 10.629 [95% CI, 3.858-29.286]; P < 0.001), stage III (HR, 0.136 [95% CI, 0.31-0.589]; P = 0.008) and perineural invasion (PNI) (HR, 8.393 [95% CI, 2.094-33.637]; P = 0.003) were independent risk factors for postoperative recurrence of stage III colon cancer.
Conclusions: The consistency between preoperative radiological and postoperative pathological staging was poor, especially for tumors located in the ascending colon and descending colon. Elastic lamina staining is expected to become a stratified indicator of recurrence risk for patients with stage III colon cancer and a guide for individualized adjuvant chemotherapy, thus improving patient prognosis.
Keywords: Colon cancer; Disease-free survival; Elastic lamina invasion; Elastic lamina staining; Recurrence risk.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
The clinical significance of elastic lamina invasion in patients with pStage II colorectal cancer: a notable prognostic indicator.World J Surg Oncol. 2024 Oct 14;22(1):274. doi: 10.1186/s12957-024-03556-6. World J Surg Oncol. 2024. PMID: 39397010 Free PMC article.
-
The prognosis significance and application value of peritoneal elastic lamina invasion in colon cancer.PLoS One. 2018 Apr 9;13(4):e0194804. doi: 10.1371/journal.pone.0194804. eCollection 2018. PLoS One. 2018. PMID: 29630617 Free PMC article.
-
Prognostic significance of additional histologic features for subclassification of pathological T3 colon cancer.Int J Clin Oncol. 2022 Sep;27(9):1428-1438. doi: 10.1007/s10147-022-02192-y. Epub 2022 Jun 18. Int J Clin Oncol. 2022. PMID: 35716324 Free PMC article.
-
Assessment of peritoneal elastic laminal invasion improves survival stratification of pT3 and pT4a colorectal cancer: a meta-analysis.J Clin Pathol. 2019 Nov;72(11):736-740. doi: 10.1136/jclinpath-2019-206056. Epub 2019 Aug 30. J Clin Pathol. 2019. PMID: 31471468 Review.
-
Special cancer microenvironment in human colonic cancer: Concept of cancer microenvironment formed by peritoneal invasion (CMPI) and implication of subperitoneal fibroblast in cancer progression.Pathol Int. 2016 Mar;66(3):123-131. doi: 10.1111/pin.12389. Epub 2016 Jan 27. Pathol Int. 2016. PMID: 26816328 Free PMC article. Review.
Cited by
-
The clinical significance of elastic lamina invasion in patients with pStage II colorectal cancer: a notable prognostic indicator.World J Surg Oncol. 2024 Oct 14;22(1):274. doi: 10.1186/s12957-024-03556-6. World J Surg Oncol. 2024. PMID: 39397010 Free PMC article.
References
-
- Siegel RL, et al. Cancer Statistics, 2021. CA Cancer J Clin. 2021. 10.3322/caac.21654.
-
- Zlobec I, Lugli A. Prognostic and predictive factors in colorectal cancer. J Clin Pathol. 2008. 10.1136/jcp.2007.054858. - PubMed
-
- Malmstrom ML, et al. Staging with computed tomography of patients with colon cancer. Int J Color Dis. 2018. 10.1007/s00384-017-2932-3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
