

Trunk Biomechanics in Individuals with Knee Disorders: A Systematic Review with Evidence Gap Map and Meta-analysis
- PMID: 36503991
- PMCID: PMC9742076
- DOI: 10.1186/s40798-022-00536-6
Trunk Biomechanics in Individuals with Knee Disorders: A Systematic Review with Evidence Gap Map and Meta-analysis
Abstract
Background: The trunk is the foundation for transfer and dissipation of forces throughout the lower extremity kinetic chain. Individuals with knee disorders may employ trunk biomechanical adaptations to accommodate forces at the knee or compensate for muscle weakness. This systematic review aimed to synthesize the literature comparing trunk biomechanics between individuals with knee disorders and injury-free controls.
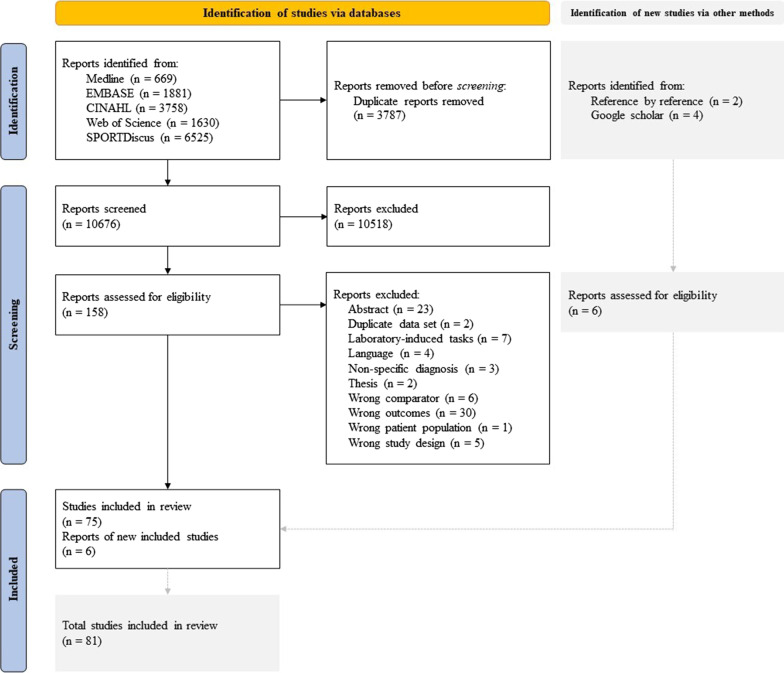
Methods: Five databases were searched from inception to January 2022. Observational studies comparing trunk kinematics or kinetics during weight-bearing tasks (e.g., stair negotiation, walking, running, landings) between individuals with knee disorders and controls were included. Meta-analyses for each knee disorder were performed. Outcome-level certainty was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE), and evidence gap maps were created.
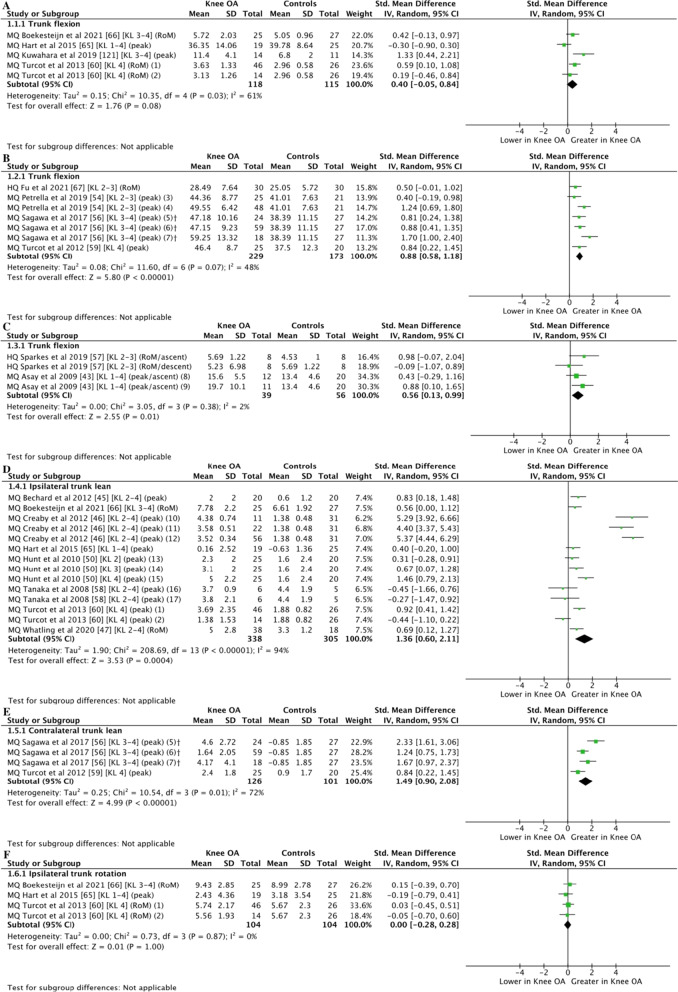
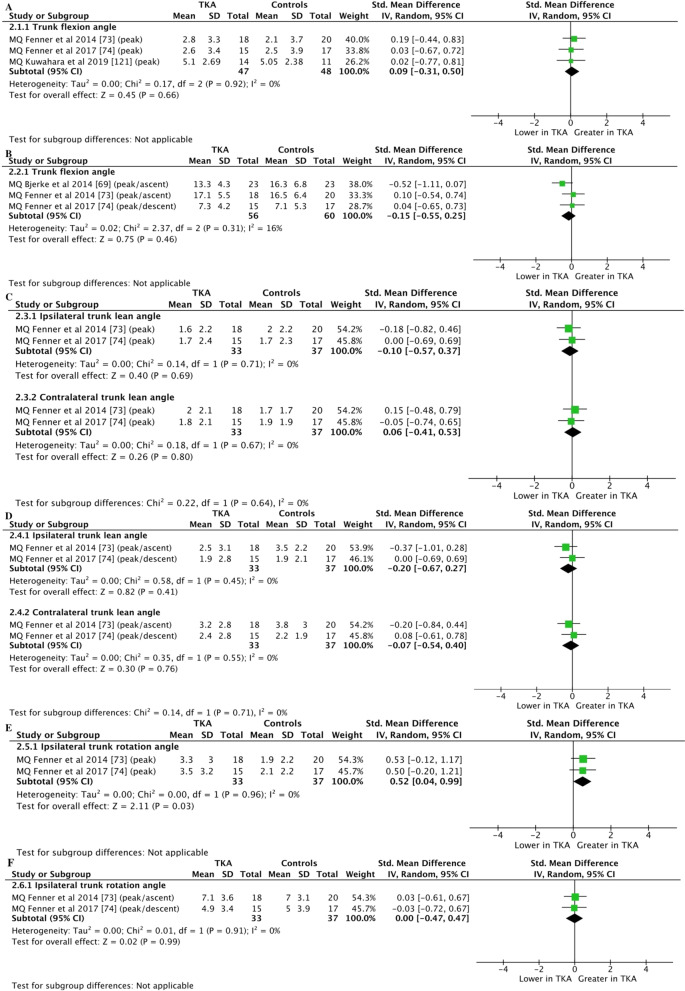
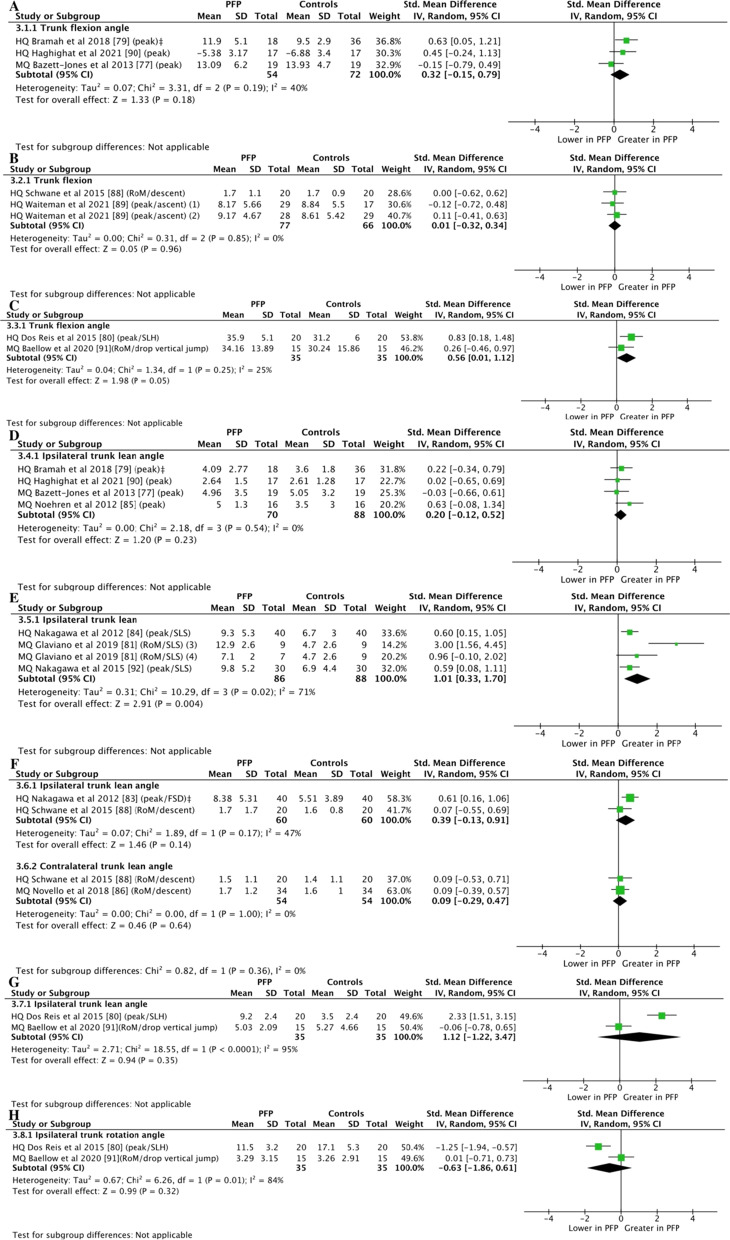
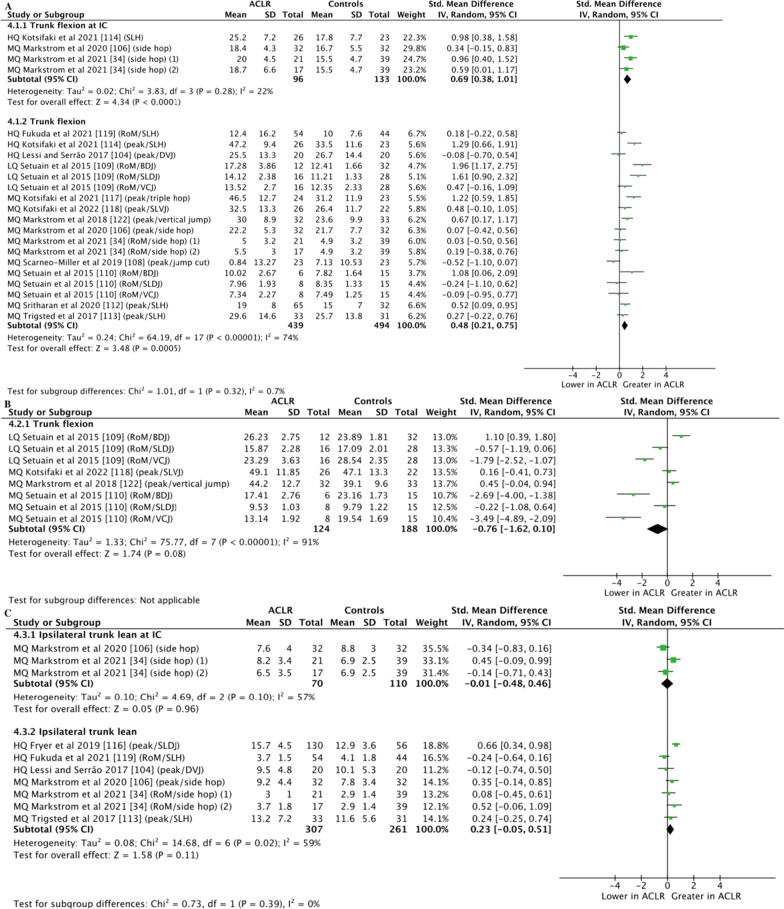
Results: A total of 81 studies investigating trunk biomechanics across six different knee disorders were included (i.e., knee osteoarthritis [OA], total knee arthroplasty [TKA], patellofemoral pain [PFP], patellar tendinopathy [PT], anterior cruciate ligament deficiency [ACLD], and anterior cruciate ligament reconstruction [ACLR]). Individuals with knee OA presented greater trunk flexion during squatting (SMD 0.88, 95% CI 0.58-1.18) and stepping tasks (SMD 0.56, 95% CI 0.13-.99); ipsilateral and contralateral trunk lean during walking (SMD 1.36; 95% CI 0.60-2.11) and sit-to-stand (SMD 1.49; 95% CI 0.90-2.08), respectively. Greater trunk flexion during landing tasks in individuals with PFP (SMD 0.56; 95% CI 0.01-1.12) or ACLR (SMD 0.48; 95% CI 0.21-.75) and greater ipsilateral trunk lean during single-leg squat in individuals with PFP (SMD 1.01; 95% CI 0.33-1.70) were also identified. No alterations in trunk kinematics of individuals with TKA were identified. Evidence gap maps outlined the lack of investigations for individuals with PT or ACLD, as well as for trunk kinetics across knee disorders.
Conclusion: Individuals with knee OA, PFP, or ACLR present with altered trunk kinematics in the sagittal and frontal planes. The findings of this review support the assessment of trunk biomechanics in these individuals in order to identify possible targets for rehabilitation and avoidance strategies.
Trial registration: PROSPERO registration number: CRD42019129257.
Keywords: Anterior cruciate ligament; Knee injuries; Knee pain; Knee surgeries; Trunk motion.
© 2022. The Author(s).
Conflict of interest statement
Marina Waiteman, Lionel Chia, Matheus Ducatti, David Bazett‑Jones, Evangelos Pappas, Fábio de Azevedo and Ronaldo Briani declare that they have no competing interests.
Figures
Similar articles
-
Progressive Changes in Walking Kinematics and Kinetics After Anterior Cruciate Ligament Injury and Reconstruction: A Review and Meta-Analysis.J Athl Train. 2017 Sep;52(9):847-860. doi: 10.4085/1062-6050-52.6.06. J Athl Train. 2017. PMID: 28985125 Free PMC article. Review.
-
Individuals With an Anterior Cruciate Ligament-Reconstructed Knee Display Atypical Whole Body Movement Strategies but Normal Knee Robustness During Side-Hop Landings: A Finite Helical Axis Analysis.Am J Sports Med. 2020 Apr;48(5):1117-1126. doi: 10.1177/0363546520910428. Epub 2020 Mar 13. Am J Sports Med. 2020. PMID: 32168459 Free PMC article.
-
Fear of Reinjury Following Anterior Cruciate Ligament Reconstruction Is Manifested in Muscle Activation Patterns of Single-Leg Side-Hop Landings.Phys Ther. 2022 Feb 1;102(2):pzab218. doi: 10.1093/ptj/pzab218. Phys Ther. 2022. PMID: 34554253 Free PMC article.
-
Kinematic and Kinetic Gait Characteristics in People with Patellofemoral Pain: A Systematic Review and Meta-analysis.Sports Med. 2023 Feb;53(2):519-547. doi: 10.1007/s40279-022-01781-1. Epub 2022 Nov 5. Sports Med. 2023. PMID: 36334239
-
Trunk, pelvis, and knee kinematics during running in females with and without patellofemoral pain.Gait Posture. 2021 Sep;89:80-85. doi: 10.1016/j.gaitpost.2021.06.023. Epub 2021 Jun 29. Gait Posture. 2021. PMID: 34246176
Cited by
-
Relationship Between the Results of the Landing Error Scoring System and Trunk Muscle Thickness.Int J Sports Phys Ther. 2024 Sep 1;19(9):1080-1087. doi: 10.26603/001c.122639. eCollection 2024. Int J Sports Phys Ther. 2024. PMID: 39229453 Free PMC article.
-
Patellar Tendon Load Progression during Rehabilitation Exercises: Implications for the Treatment of Patellar Tendon Injuries.Med Sci Sports Exerc. 2024 Mar 1;56(3):545-552. doi: 10.1249/MSS.0000000000003323. Epub 2023 Oct 16. Med Sci Sports Exerc. 2024. PMID: 37847102 Free PMC article.
-
Efficacy of Mulligan joint mobilizations and trunk stabilization exercises versus isometric knee strengthening in the management of knee osteoarthritis: a randomized controlled trial.BMC Sports Sci Med Rehabil. 2024 May 7;16(1):105. doi: 10.1186/s13102-024-00893-7. BMC Sports Sci Med Rehabil. 2024. PMID: 38715135 Free PMC article.
-
Detection of kinematic abnormalities in persons with knee osteoarthritis using markerless motion capture during functional movement screen and daily activities.Front Bioeng Biotechnol. 2024 Feb 5;12:1325339. doi: 10.3389/fbioe.2024.1325339. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38375453 Free PMC article.
-
People With Patellofemoral Pain Have Bilateral Deficits in Physical Performance Regardless of Pain Laterality.J Athl Train. 2024 Nov 1;59(11):1110-1117. doi: 10.4085/1062-6050-0649.23. J Athl Train. 2024. PMID: 38477146
References
-
- Lankhorst NE, van Middelkoop M, Crossley KM, Bierma-Zeinstra SMA, Oei EHG, Vicenzino B, et al. Factors that predict a poor outcome 5–8 years after the diagnosis of patellofemoral pain: a multicentre observational analysis. Br J Sports Med. 2015;50:881–886. doi: 10.1136/bjsports-2015-094664. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
