

EASY-WPW: a novel ECG-algorithm for easy and reliable localization of manifest accessory pathways in children and adults
- PMID: 36504238
- PMCID: PMC9935024
- DOI: 10.1093/europace/euac216
EASY-WPW: a novel ECG-algorithm for easy and reliable localization of manifest accessory pathways in children and adults
Abstract
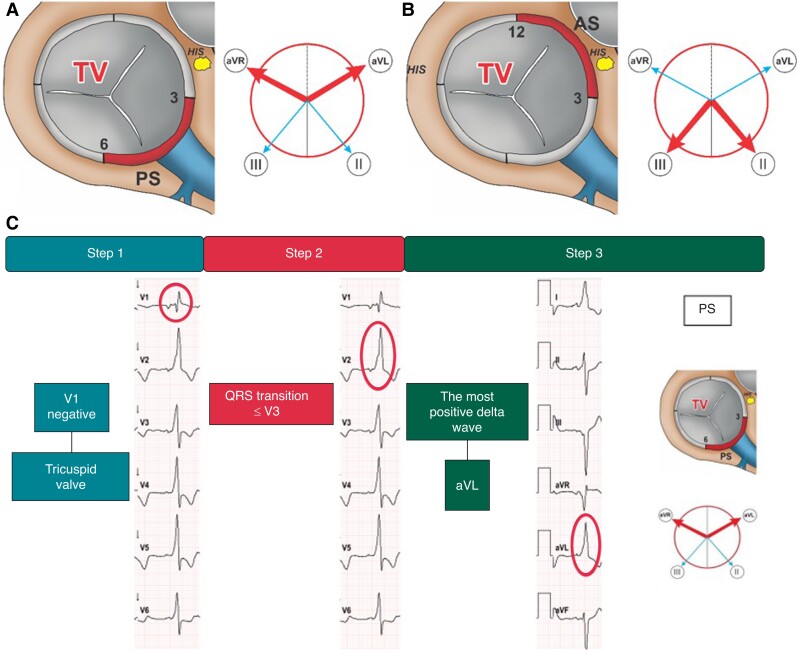
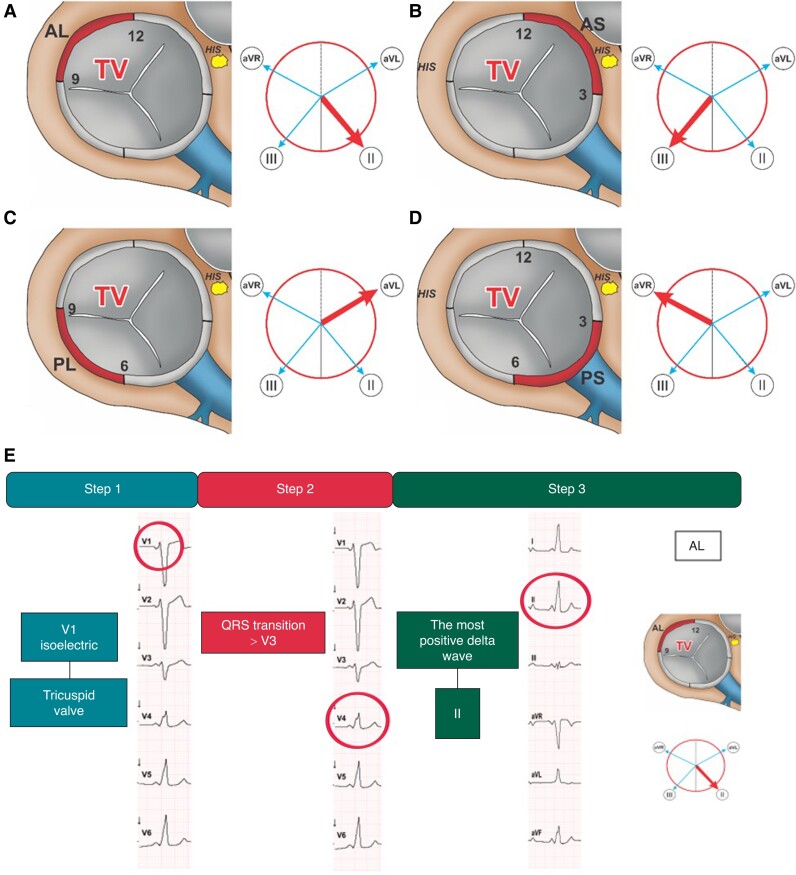
Aims: Accessory pathway (AP) ablation is a standard procedure for the treatment of Wolff-Parkinson-White syndrome (WPW). Twelve-lead electrocardiogram (ECG)-based delta wave analysis is essential for predicting ablation sites. Previous algorithms have shown to be complex, time-consuming, and unprecise. We aimed to retrospectively develop and prospectively validate a new, simple ECG-based algorithm considering the patients' heart axis allowing for exact localization of APs in patients undergoing ablation for WPW.
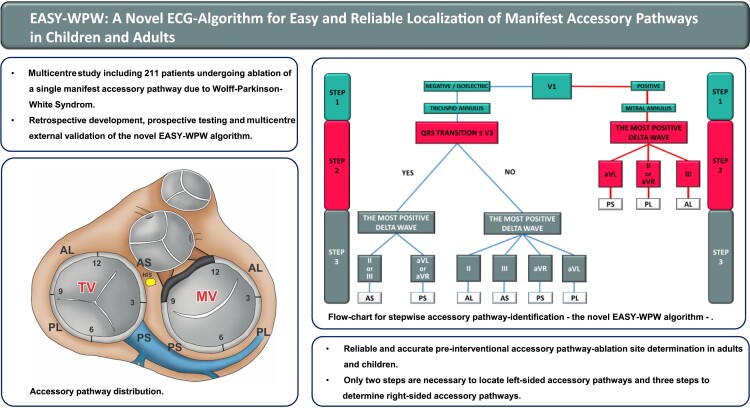
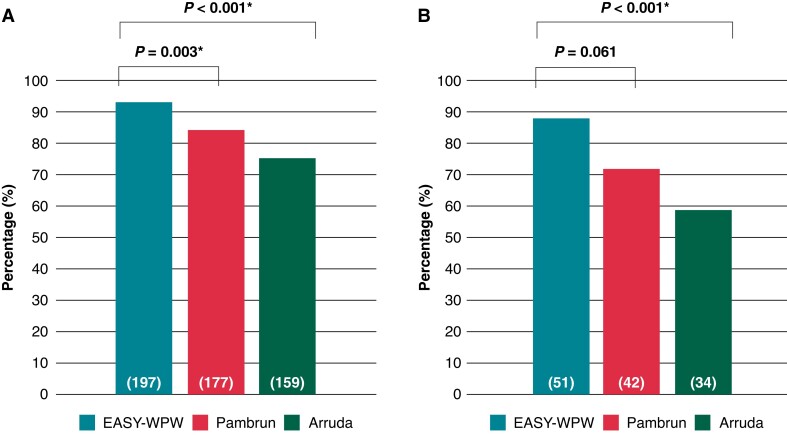
Methods and results: Our multicentre study included 211 patients undergoing ablation of a single manifest AP due to WPW between 2013 and 2021. The algorithm was developed retrospectively and validated prospectively by comparing its efficacy to two established ones (Pambrun and Arruda). All patients (32 ± 19 years old, 47% female) underwent successful pathway ablation. Prediction of AP-localization was correct in 197 patients (93%) (sensitivity 92%, specificity 99%, PPV 96%, and NPV 99%). Our algorithm was particularly useful in correctly localizing antero-septal/-lateral (sensitivity and specificity 100%) and posteroseptal (sensitivity 98%, specificity 92%) AP in proximity to the tricuspid valve. The accuracy of EASY-WPW was superior compared to the Pambrun (93% vs. 84%, P = 0.003*) and the Arruda algorithm (94% vs. 75%, P < 0.001*). A subgroup analysis of children (n = 58, 12 ± 4 years old, 55% female) revealed superiority to the Arruda algorithm (P < 0.001*). The reproducibility of our algorithm was excellent (ϰ>0.8; P < 0.001*).
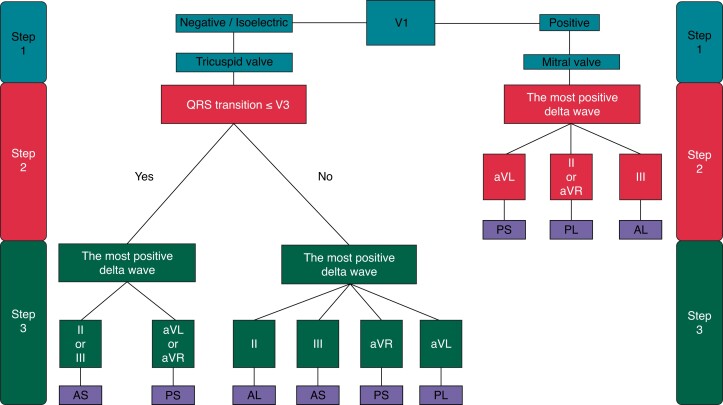
Conclusion: The novel EASY-WPW algorithm provides reliable and accurate pre-interventional ablation site determination in WPW patients. Only two steps are necessary to locate left-sided AP, and three steps to determine right-sided AP.
Keywords: Accessory pathway localization; Algorithm; Catheter ablation; Electrocardiography; Wolff-Parkinson-White syndrome.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Philipp Sommer is member of the advisory board of Abbott, Biosense Webster, Boston Scientific and Medtronic. Christian Heeger is member of the advisory board of Biosense Webster. The other authors have nothing to declare.
Figures
References
-
- Antz M, Weiss C, Volkmer M, Hebe J, Ernst S, Ouyang Fet al. . Risk of sudden death after successful accessory atrioventricular pathway ablation in resuscitated patients with Wolff-Parkinson-White syndrome. J Cardiovasc Electrophysiol 2002;13:231–6. - PubMed
-
- Derejko P, Szumowski LJ, Sanders P, Krupa W, Bodalski R, Orczykowski Met al. . Atrial fibrillation in patients with Wolff-Parkinson-White syndrome: role of pulmonary veins. J Cardiovasc Electrophysiol 2012;23:280–6. - PubMed
-
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist Cet al. . 2019 ESC guidelines for the management of patients with supraventricular tachycardia. The task force for the management of patients with supraventricular tachycardia of the European society of cardiology (ESC). Eur Heart J 2020;41:655–720. - PubMed
-
- Arruda MS, McClelland JH, Wang X, Beckman KJ, Widman LE, Gonzalez MDet al. . Development and validation of an ECG algorithm for identifying accessory pathway ablation site in Wolff-Parkinson-White syndrome. J Cardiovasc Electrophysiol 1998;9:2–12. - PubMed
-
- Fitzpatrick AP, Gonzales RP, Lesh MD, Modin GW, Lee RJ, Scheinman MM. New algorithm for the localization of accessory atrioventricular connections using a baseline electrocardiogram. J Am Coll Cardiol 1994;23:107–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
