

Development of a warning score for early detection of colorectal anastomotic leakage: Hype or hope?
- PMID: 36504511
- PMCID: PMC9727571
- DOI: 10.4240/wjgs.v14.i11.1297
Development of a warning score for early detection of colorectal anastomotic leakage: Hype or hope?
Abstract
Background: Colorectal anastomotic leakage (CAL), a severe postoperative complication, is associated with high morbidity, hospital readmission, and overall healthcare costs. Early detection of CAL remains a challenge in clinical practice. However, some decision models have been developed to increase the diagnostic accuracy of this event.
Aim: To develop a score based on easily accessible variables to detect CAL early.
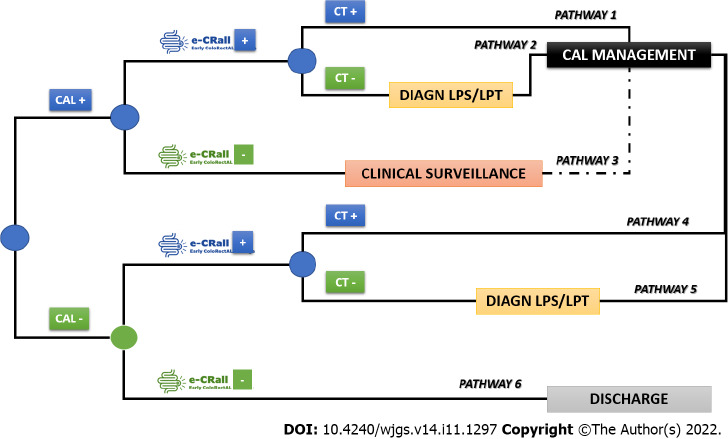
Methods: Based on the least absolute shrinkage and selection operator method, a predictive classification system was developed [Early ColoRectAL Leakage (E-CRALL) score] from a prospective observational, single center cohort, carried out in a colorectal division from a non-academic hospital. The score performance and CAL threshold from postoperative day (POD) 3 to POD5 were estimated. Based on a precise analytical decision model, the standard clinical practice was compared with the E-CRALL adoption on POD3, POD4, or POD5. A cost-minimization analysis was conducted, on the assumption that all alternatives delivered similar health-related effects.
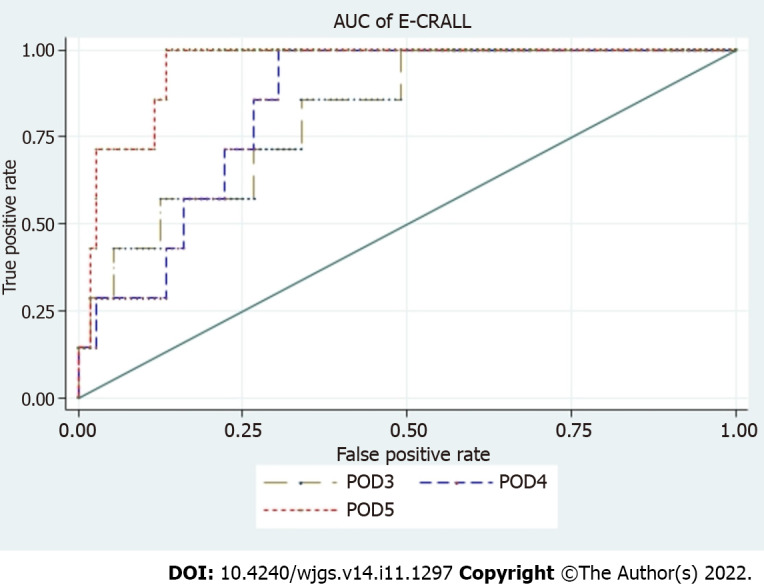
Results: In this study, 396 patients who underwent colorectal resection surgery with anastomosis, and 6.3% (n = 25) developed CAL. Most of the patients who developed CAL (n = 23; 92%) were diagnosed during the first hospital admission, with a median time of diagnosis of 9.0 ± 6.8 d. From POD3 to POD5, the area under the receiver operating characteristic curve of the E-CRALL score was 0.82, 0.84, and 0.95, respectively. On POD5, if a threshold of 8.29 was chosen, 87.4% of anastomotic failures were identified with E-CRALL adoption. Additionally, score usage could anticipate CAL diagnosis in an average of 5.2 d and 4.1 d, if used on POD3 and POD5, respectively. Regardless of score adoption, episode comprehensive costs were markedly greater (up to four times) in patients who developed CAL in comparison with patients who did not develop CAL. Nonetheless, the use of the E-CRALL warning score was associated with cost savings of €421442.20, with most (92.9%) of the savings from patients who did not develop CAL.
Conclusion: The E-CRALL score is an accessible tool to predict CAL at an early timepoint. Additionally, E-CRALL can reduce overall healthcare costs, mainly in the reduction of hospital costs, independent of whether a patient developed CAL.
Keywords: Anastomotic leakage; Biomarkers; Colorectal; Costs; Score; Surgery.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Usefulness of serum C-reactive protein and calprotectin for the early detection of colorectal anastomotic leakage: A prospective observational study.World J Gastroenterol. 2022 Jun 28;28(24):2758-2774. doi: 10.3748/wjg.v28.i24.2758. World J Gastroenterol. 2022. PMID: 35979163 Free PMC article.
-
Peritoneal and Systemic Interleukin-10 as Early Biomarkers for Colorectal Anastomotic Leakage Following Surgery in Colorectal Cancer Patients: A Systematic Review and Meta-Analysis.Pol Przegl Chir. 2023 Nov 16;96(0):135-142. doi: 10.5604/01.3001.0053.9836. Pol Przegl Chir. 2023. PMID: 38348991
-
Peritoneal Cytokines as Early Biomarkers of Colorectal Anastomotic Leakage Following Surgery for Colorectal Cancer: A Meta-Analysis.Front Oncol. 2022 Jan 21;11:791462. doi: 10.3389/fonc.2021.791462. eCollection 2021. Front Oncol. 2022. PMID: 35127496 Free PMC article.
-
[The clinical values of neutrophil-to-lymphocyte ratio as an early predictor of anastomotic leak in postoperative rectal cancer patients].Zhonghua Zhong Liu Za Zhi. 2020 Jan 23;42(1):70-73. doi: 10.3760/cma.j.issn.0253-3766.2020.01.011. Zhonghua Zhong Liu Za Zhi. 2020. PMID: 32023773 Chinese.
-
Bilirubin, urobilinogen, pancreas elastase and bile acid in drain fluid. The GBUP-study: Analysis of biomarkers for a colorectal anastomotic leakage.Ann Med Surg (Lond). 2018 Sep 21;35:44-50. doi: 10.1016/j.amsu.2018.09.008. eCollection 2018 Nov. Ann Med Surg (Lond). 2018. PMID: 30294427 Free PMC article.
References
-
- Lee SW, Gregory D, Cool CL. Clinical and economic burden of colorectal and bariatric anastomotic leaks. Surg Endosc. 2020;34:4374–4381. - PubMed
-
- La Regina D, Di Giuseppe M, Lucchelli M, Saporito A, Boni L, Efthymiou C, Cafarotti S, Marengo M, Mongelli F. Financial Impact of Anastomotic Leakage in Colorectal Surgery. J Gastrointest Surg. 2019;23:580–586. - PubMed
-
- Lagoutte N, Facy O, Ravoire A, Chalumeau C, Jonval L, Rat P, Ortega-Deballon P. C-reactive protein and procalcitonin for the early detection of anastomotic leakage after elective colorectal surgery: pilot study in 100 patients. J Visc Surg. 2012;149:e345–e349. - PubMed
-
- den Dulk M, Witvliet MJ, Kortram K, Neijenhuis PA, de Hingh IH, Engel AF, van de Velde CJ, de Brauw LM, Putter H, Brouwers MA, Steup WH. The DULK (Dutch leakage) and modified DULK score compared: actively seek the leak. Colorectal Dis. 2013;15:e528–e533. - PubMed
LinkOut - more resources
Full Text Sources
