

Global burden of calcific aortic valve disease and attributable risk factors from 1990 to 2019
- PMID: 36505369
- PMCID: PMC9727398
- DOI: 10.3389/fcvm.2022.1003233
Global burden of calcific aortic valve disease and attributable risk factors from 1990 to 2019
Abstract
Background: Calcific aortic valve disease (CAVD) was highly prevalent among developed countries and caused numerous deaths. Based on the Global Burden of Disease 2019, this study was designed to present comprehensive epidemiological information, attributable risks, and relevant factors.
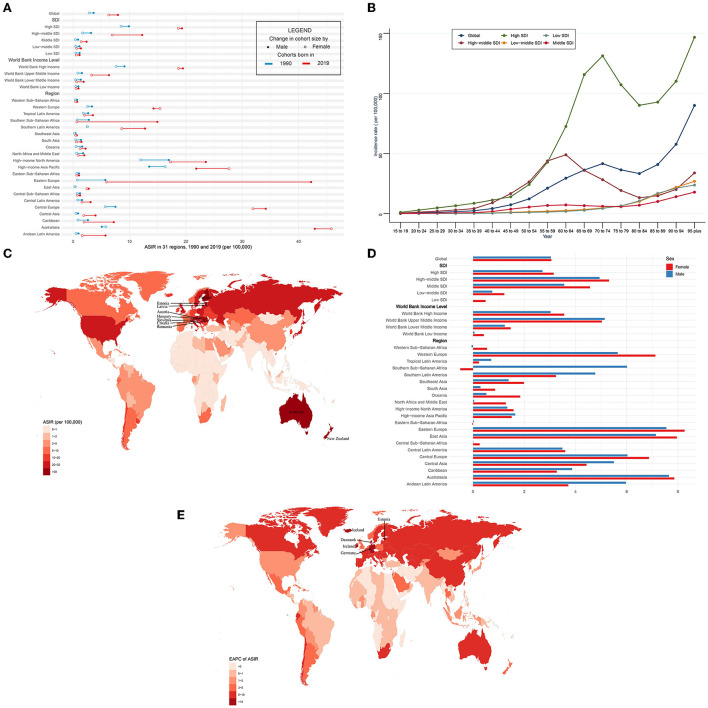
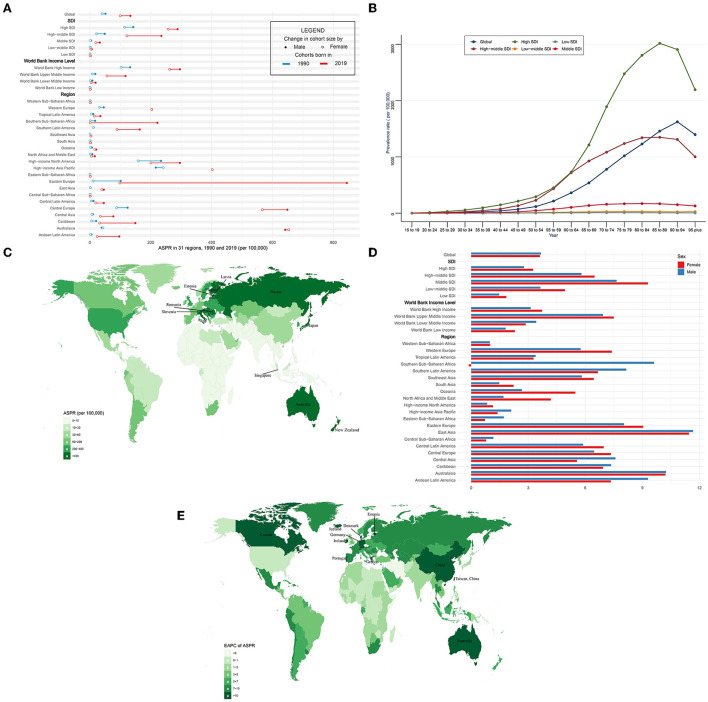
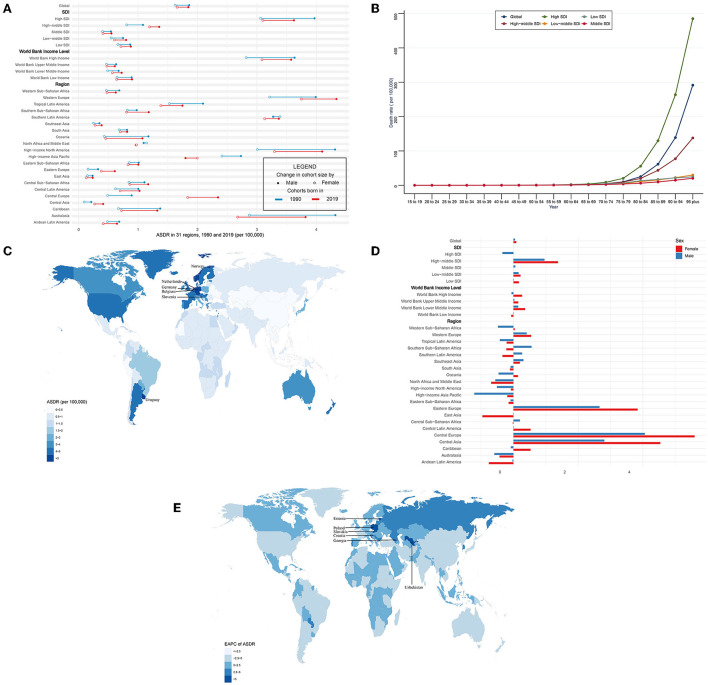
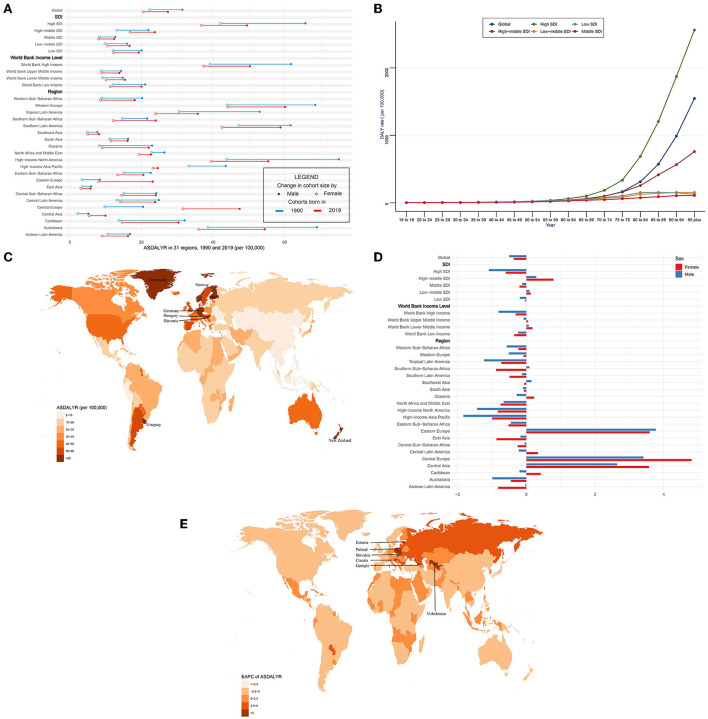
Methods: All data were available online via the Global Health Data Exchange (GHDx). In this study, we analyzed the global incidence, prevalence, deaths, and disability-adjusted life years (DALYs) of CAVD across different regions from 1990 to 2019. We applied the estimated annual percentage changes (EAPCs) to evaluate the change trends and their attributable risks. In addition, we explored several relevant factors.
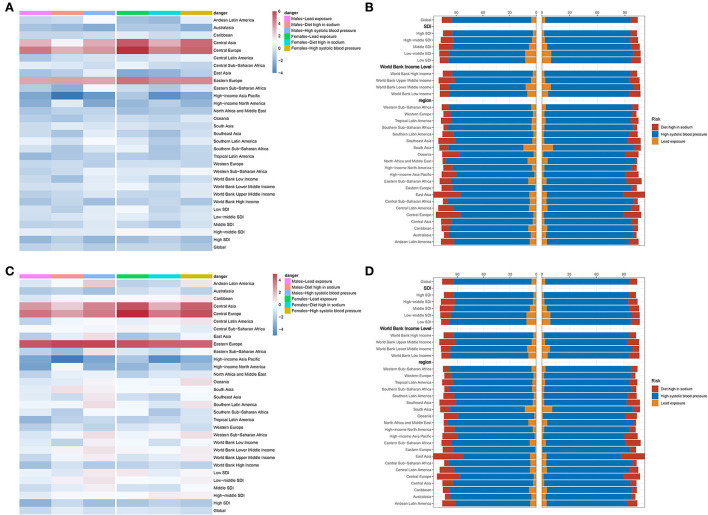
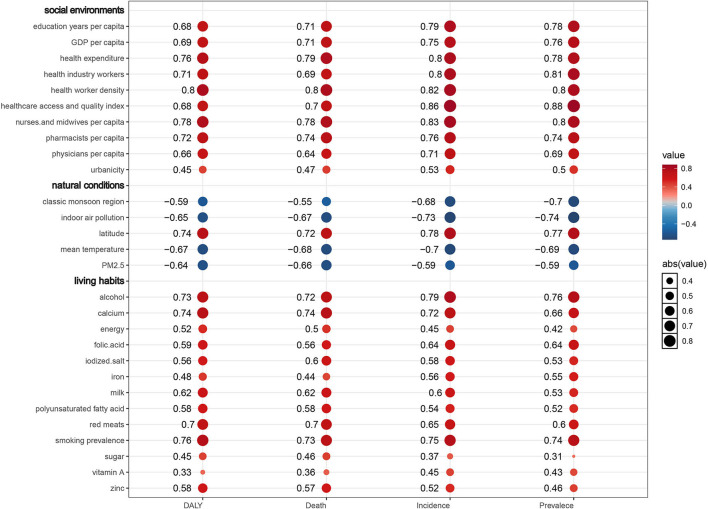
Results: From 1990 to 2019, the incidence cases, prevalence cases, CAVD-related deaths, and DALYs of CAVD gradually increased globally. However, the age-standardized death rate (ASDR) was relatively stable, and the age-standardized DALYs rate gradually declined during the past 30 years. Males and elderly individuals were more likely to suffer from CAVD. High systolic blood pressure (SBP) was the predominant attributable risk of disease burden that presented a global downward trend (death: EAPC = -0.68, 95% CI -0.77~-0.59, P < 0.001; DALYs: EAPC = -0.99, 95% CI -1.09 to -0.89, P < 0.001). Alcohol consumption (R = 0.79, P < 0.001), smoking prevalence (R = 0.75, P < 0.001), and calcium (R = 0.72, P < 0.001) showed a positive correlation with the age-standardized incidence rate (ASIR), whereas classic monsoon region (R = -0.68, P < 0.001) and mean temperature (R = -0.7, P < 0.001) showed a negative correlation with age-standardized incidence rate (ASIR). Besides, medical and healthcare resources presented a positive correlation with ASIR. Meanwhile, similar relationships were found in age-standardized prevalence rate (ASPR), ASDR, and age-standardized DALY rate (ASDALYR).
Conclusion: CAVD displays widely varied spatial distribution around the world, of which high SDI regions have the highest burdens. Age is a powerful factor and hypertension a predominant attributable risk factor. Moreover, controlling blood pressure, avoiding smoking, reducing alcohol consumption, and so on, could effectively reduce the burden of CAVD.
Keywords: Global Burden of Disease Study; attributable risk factor; calcific aortic valve disease; disability-adjusted life year; estimated annual percentage change.
Copyright © 2022 Yu, Wang, Bao, Lei, You, Yin and Xie.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. . Executive summary: heart disease and stroke statistics-−2013 update: a report from the American Heart Association. Circulation. (2013) 127:143–52. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous