

A retrospective review of antibiotic use for acute respiratory infections in urgent-care patients
- PMID: 36505944
- PMCID: PMC9727505
- DOI: 10.1017/ash.2022.337
A retrospective review of antibiotic use for acute respiratory infections in urgent-care patients
Abstract
Objective: We examined the use of antibiotics for acute respiratory infections in an urgent-care setting.
Design: Retrospective database review.
Setting: The study was conducted in 2 urgent-care clinics staffed by academic emergency physicians in San Diego, California.
Patients: Visits for acute respiratory infections were identified based on presenting complaints.
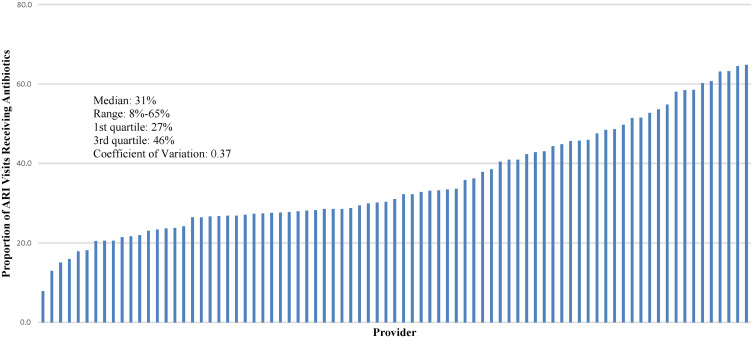
Methods: The primary outcome was a discharge prescription for an antibiotic. The patient and provider characteristics that predicted this outcome were analyzed using logistic regression. The variation in antibiotic prescriptions between providers was also analyzed.
Results: In total, 15,160 visits were analyzed. The patient characteristics were not predictive of antibiotic treatment. Physicians were more likely than advanced practice practitioners to prescribe antibiotics (1.31; 95% confidence interval [CI], 1.21-1.42). For every year of seniority, a provider was 1.03 (95% CI, 1.02-1.03) more likely to prescribe an antibiotic. Although the providers saw similar patients, we detected significant variation in the antibiotic prescription rate between providers: the mean antibiotic prescription rate within the top quartile was 54.3% and the mean rate in the bottom quartile was 21.7%.
Conclusions: The patient and provider characteristics we examined were either not predictive or were only weakly predictive of receiving an antibiotic prescription for acute respiratory infection. However, we detected a marked variation between providers in the rate of antibiotic prescription. Provider differences, not patient differences, drive variations in antibiotic prescriptions. Stewardship efforts may be more effective if directed at providers rather than patients.
© The Author(s) 2022.
Figures
Similar articles
-
Variation in Outpatient Antibiotic Prescribing for Acute Respiratory Infections in the Veteran Population: A Cross-sectional Study.Ann Intern Med. 2015 Jul 21;163(2):73-80. doi: 10.7326/M14-1933. Ann Intern Med. 2015. PMID: 26192562
-
Variability in Antibiotic Prescribing for Upper Respiratory Illnesses by Provider Specialty.J Pediatr. 2018 Dec;203:76-85.e8. doi: 10.1016/j.jpeds.2018.07.044. Epub 2018 Sep 5. J Pediatr. 2018. PMID: 30195553
-
Antibiotic Prescribing Practices for Upper Respiratory Tract Infections Among Primary Care Providers: A Descriptive Study.Open Forum Infect Dis. 2022 Jun 17;9(7):ofac302. doi: 10.1093/ofid/ofac302. eCollection 2022 Jul. Open Forum Infect Dis. 2022. PMID: 35891692 Free PMC article.
-
Antibiotic prescribing for acute respiratory tract infections in the United States outpatient setting.BMC Fam Pract. 2019 Jul 2;20(1):91. doi: 10.1186/s12875-019-0980-1. BMC Fam Pract. 2019. PMID: 31266449 Free PMC article.
-
Patient, Provider, and Practice Characteristics Associated with Inappropriate Antimicrobial Prescribing in Ambulatory Practices.Infect Control Hosp Epidemiol. 2018 Mar;39(3):307-315. doi: 10.1017/ice.2017.263. Epub 2018 Jan 30. Infect Control Hosp Epidemiol. 2018. PMID: 29378672
References
-
- Spellberg B, Guidos R, Gilbert D, et al. The epidemic of antibiotic-resistant infections: a call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis 2008;46:155–164. - PubMed
-
- Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol 2012;33:322–327. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016;315:1864–1873. - PubMed
-
- Ahovuo-Saloranta A, Rautakorpi UM, Borisenko OV, Liira H, Williams JW Jr, Makela M. Antibiotics for acute maxillary sinusitis in adults. Cochrane Database Syst Rev 2014;2:CD000243. - PubMed
LinkOut - more resources
Full Text Sources