

A nomogram for evaluation and analysis of difficulty in retroperitoneal laparoscopic adrenalectomy: A single-center study with prospective validation using LASSO-logistic regression
- PMID: 36506074
- PMCID: PMC9732249
- DOI: 10.3389/fendo.2022.1004112
A nomogram for evaluation and analysis of difficulty in retroperitoneal laparoscopic adrenalectomy: A single-center study with prospective validation using LASSO-logistic regression
Abstract
Background: While it is known that inaccurate evaluation for retroperitoneal laparoscopic adrenalectomy (RPLA) can affect the surgical results of patients, no stable and effective prediction model for the procedure exists. In this study, we aimed to develop a computed tomography (CT) -based radiological-clinical prediction model for evaluating the surgical difficulty of RPLA.
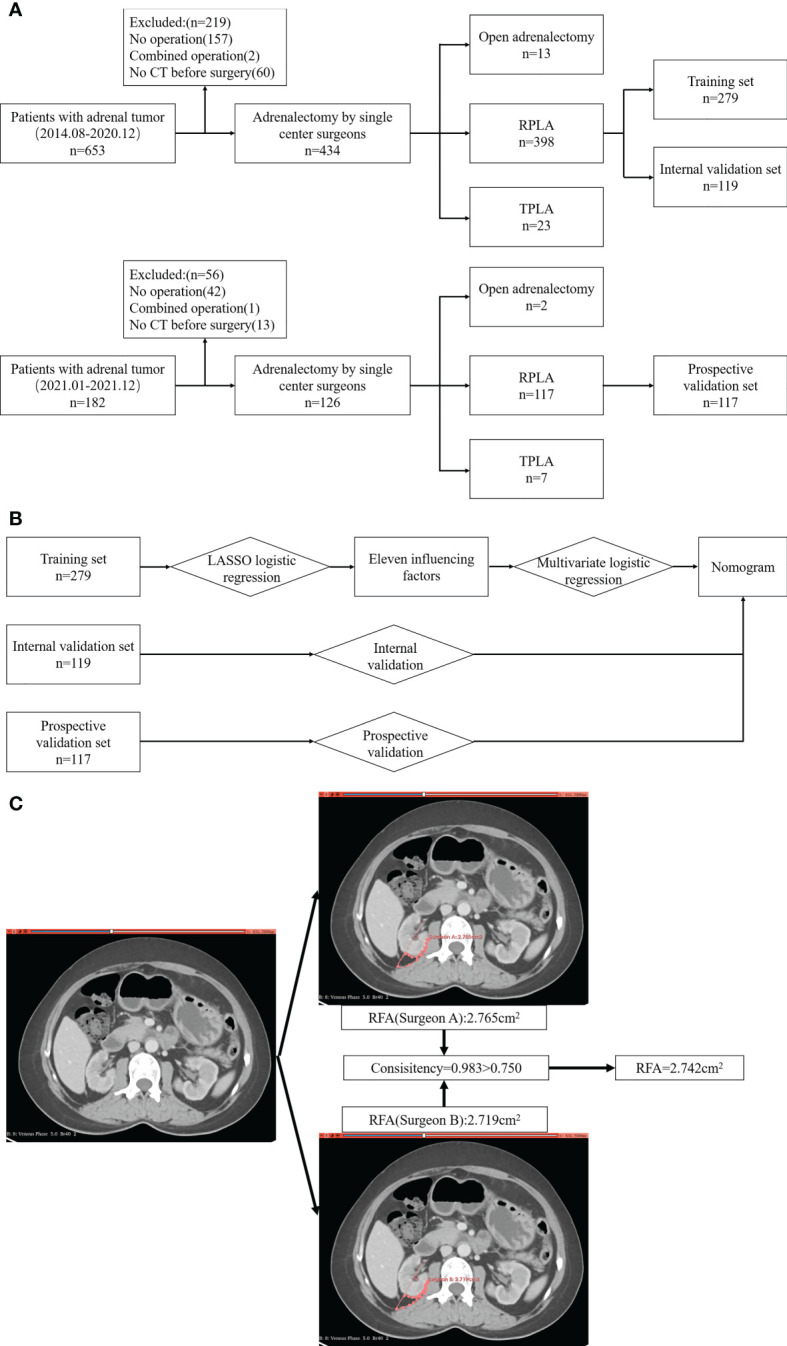
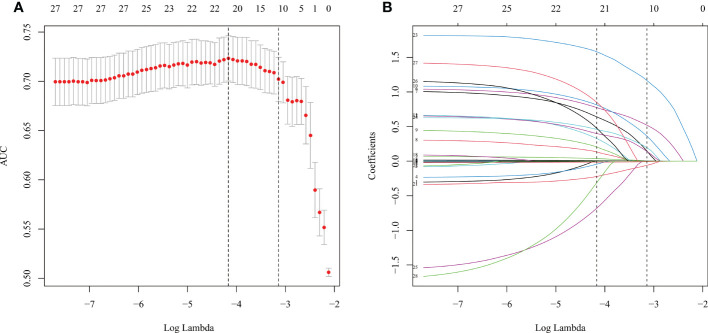
Method: Data from 398 patients with adrenal tumors treated by RPLA in a single center from August 2014 to December 2020 were retrospectively analyzed and divided into sets. The influencing factors were selected by least absolute shrinkage and selection operator regression model (LASSO). Additionally, the nomogram was constructed. A receiver operating characteristic curve was used to analyze the prediction efficiency of the nomogram. The C-index and bootstrap self-sampling methods were used to verify the discrimination and consistency of the nomogram.
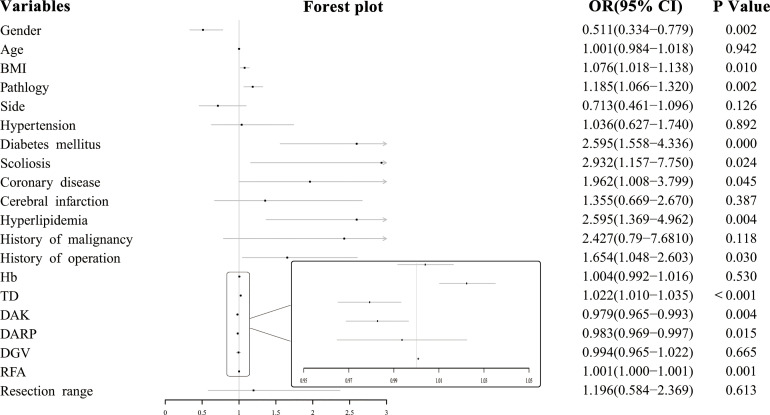
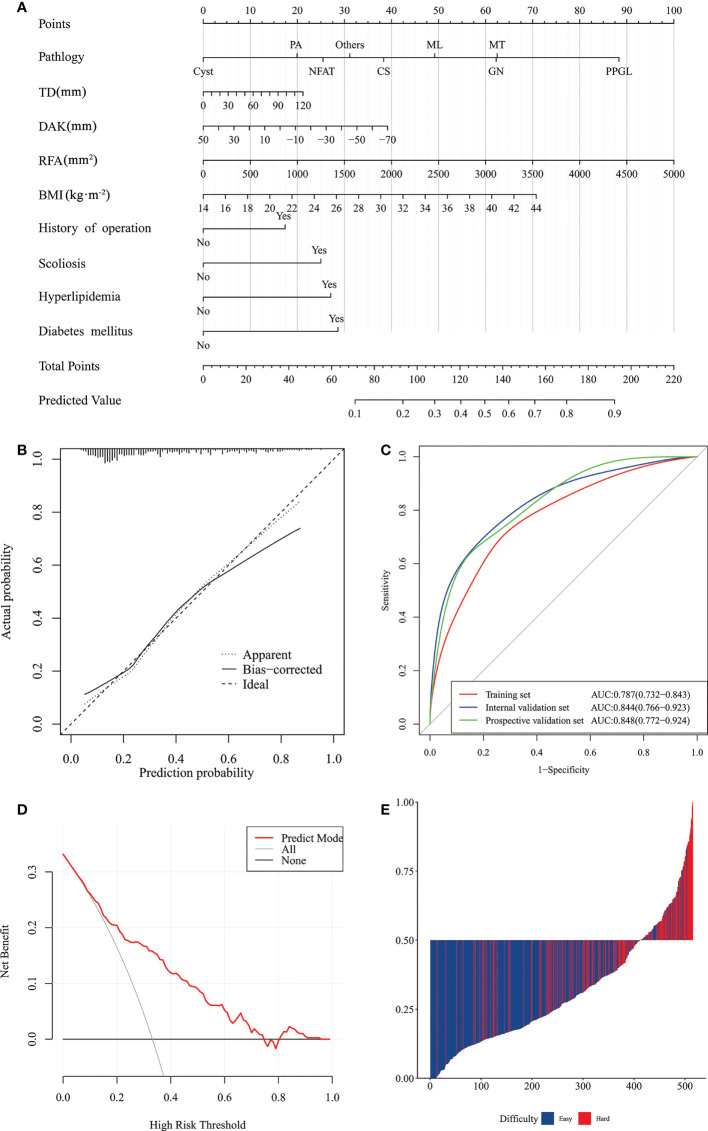
Result: The following 11 independent influencing factors were selected by LASSO: body mass index, diabetes mellitus, scoliosis, hyperlipidemia, history of operation, tumor diameter, distance from adrenal tumor to upper pole of kidney, retro renal fat area, hyperaldosteronism, pheochromocytoma and paraganglioma, and myelolipoma. The area under the curve (AUC) of the training set was 0.787, and 0.844 in the internal validation set. Decision curve analyses indicated the model to be useful. An additional 117 patients were recruited for prospective validation, and AUC was 0.848.
Conclusion: This study developed a radiological-clinical prediction model proposed for predicting the difficulty of RPLA procedures. This model was suitable, accessible, and helpful for individualized surgical preparation and reduced operational risk. Thus, this model could contribute to more patients' benefit in circumventing surgical difficulties because of accurate predictive abilities.
Keywords: LASSO; adrenalectomy; laparoscopy; nomogram; retroperitoneal space.
Copyright © 2022 Sun, Wang, Yang, Wang, Yao, Yue, Niu, Feng, Zhang, Yan, Cheng and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Development and validation of machine-learning models for the difficulty of retroperitoneal laparoscopic adrenalectomy based on radiomics.Front Endocrinol (Lausanne). 2023 Nov 16;14:1265790. doi: 10.3389/fendo.2023.1265790. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38034013 Free PMC article.
-
Establishment and validation of a nomogram for predicting the surgical difficulty of lateral retroperitoneal laparoscopic adrenalectomy.Transl Androl Urol. 2023 Jan 30;12(1):9-18. doi: 10.21037/tau-22-324. Epub 2022 Jan 3. Transl Androl Urol. 2023. PMID: 36760870 Free PMC article.
-
Establishment and validation of a nomogram for predicting perioperative complications of retroperitoneal laparoscopic adrenalectomy.Transl Androl Urol. 2023 Apr 28;12(4):572-585. doi: 10.21037/tau-22-705. Epub 2023 Apr 4. Transl Androl Urol. 2023. PMID: 37181241 Free PMC article.
-
A Nomogram for Predicting Intraoperative Hemodynamic Instability in Patients With Pheochromocytoma.Front Endocrinol (Lausanne). 2022 Jan 6;12:787786. doi: 10.3389/fendo.2021.787786. eCollection 2021. Front Endocrinol (Lausanne). 2022. PMID: 35069440 Free PMC article.
-
Laparoscopic retroperitoneal adrenalectomy.Surg Laparosc Endosc Percutan Tech. 2011 Aug;21(4):243-7. doi: 10.1097/SLE.0b013e3182266a86. Surg Laparosc Endosc Percutan Tech. 2011. PMID: 21857472 Review.
Cited by
-
Development and construction of a cataract risk prediction model based on biochemical indices: the National Health and Nutrition Examination Survey, 2005-2008.Front Med (Lausanne). 2024 Oct 21;11:1452756. doi: 10.3389/fmed.2024.1452756. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39497845 Free PMC article.
-
Development and validation of nomograms to predict survival of neuroendocrine carcinoma in genitourinary system: A population-based retrospective study.PLoS One. 2024 Jun 5;19(6):e0303440. doi: 10.1371/journal.pone.0303440. eCollection 2024. PLoS One. 2024. PMID: 38837985 Free PMC article.
-
Development and validation of nomograms to predict survival of primary adrenal lymphoma: a population-based retrospective study.Sci Rep. 2023 Sep 2;13(1):14428. doi: 10.1038/s41598-023-41839-2. Sci Rep. 2023. PMID: 37660207 Free PMC article.
-
Development and validation of machine-learning models for the difficulty of retroperitoneal laparoscopic adrenalectomy based on radiomics.Front Endocrinol (Lausanne). 2023 Nov 16;14:1265790. doi: 10.3389/fendo.2023.1265790. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38034013 Free PMC article.
-
Development and validation of nomograms to predict survival of primary cervical lymphoma: A surveillance, epidemiology, and end results (SEER) database analysis.Medicine (Baltimore). 2024 Jun 14;103(24):e38528. doi: 10.1097/MD.0000000000038528. Medicine (Baltimore). 2024. PMID: 38875393 Free PMC article.
References
-
- Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. . Management of adrenal incidentalomas: European society of endocrinology clinical practice guideline in collaboration with the European network for the study of adrenal tumors. Eur J Endocrinol (2016) 175:G1–34. doi: 10.1530/EJE-16-0467 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical