

Oozing-type rupture caused by right ventricular intramural hematoma after right ventricular infarction
- PMID: 36506502
- PMCID: PMC9727562
- DOI: 10.1016/j.jccase.2022.08.008
Oozing-type rupture caused by right ventricular intramural hematoma after right ventricular infarction
Abstract
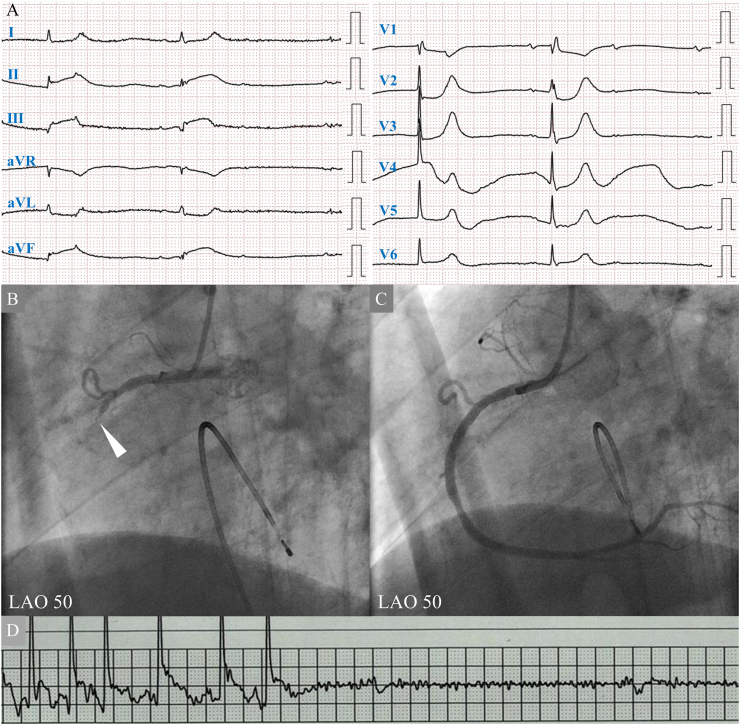
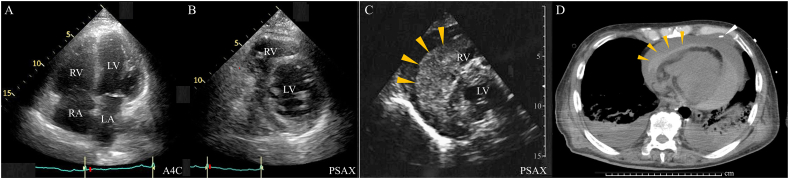
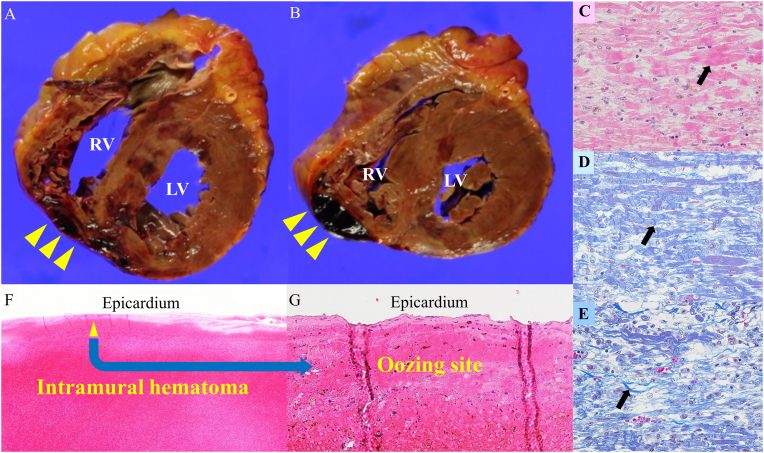
An 81-year-old man was admitted to the hospital because of decreased level of consciousness. He had bradycardia (27 beats/min). Electrocardiography showed ST-segment elevation in leads II, III, and aVF and ST-segment depression in leads aVL, V1. Transthoracic echocardiography (TTE) visualized reduced motion of the left ventricular (LV) inferior wall and right ventricular (RV) free wall. Coronary angiography revealed occlusion of the right coronary artery. A primary percutaneous coronary intervention was successfully performed with temporary pacemaker backup. On the third day, the sinus rhythm recovered, and the temporary pacemaker was removed. On the fifth day, a sudden cardiac arrest occurred. Extracorporeal cardiopulmonary resuscitation was performed. TTE showed a high-echoic effusion around the right ventricle, indicating a hematoma. The drainage was ineffective. He died on the eighth day. An autopsy showed the infarcted lesion and an intramural hematoma in the RV. However, no definite perforation of the myocardium was detected. The hematoma extended to the epicardium surface, indicative of oozing-type RV rupture induced by RV infarction. The oozing-type rupture induced by RV infarction might develop asymptomatically without influence on the vital signs of the patient. Frequent echocardiographic evaluation is essential in cases of RV infarction taking care of silent oozing-type rupture.
Learning objective: Inferior left ventricular infarction sometimes complicates right ventricular (RV) infarction. The typical manifestations of RV infarction include low blood pressure, low cardiac output, and elevated right atrium pressure. Although the frequency is low, fatal complications of oozing-type RV rupture might progress asymptomatically. Frequent echocardiographic screening is necessary to detect them.
Keywords: Cardiac arrest; Intramural hematoma; Oozing-type right ventricular rupture; Primary percutaneous coronary intervention; Right ventricular infarction; Transthoracic echocardiography.
© 2022 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Yukie Sano, Toshimitsu Kato, Noriaki Takama, Etsuko Hisanaga, Naohiro Matsumoto, Shiro Amanai, Youhei Ishibashi, Kazuhumi Aihara, Takashi Nagasaka, Norimichi Koitabashi, Yoshiaki Kaneko, Hideaki Yokoo, and Hideki Ishii declare that they have no conflicts of interest.
Figures
Similar articles
-
Right ventricular rupture induced by cardiopulmonary resuscitation.J Cardiol Cases. 2009 Nov 8;1(1):e42-e44. doi: 10.1016/j.jccase.2009.07.006. eCollection 2010 Feb. J Cardiol Cases. 2009. PMID: 30615749 Free PMC article.
-
Right Ventricular Free Wall Rupture After Myocardial Infarction.JACC Case Rep. 2021 Oct 20;3(14):1622-1624. doi: 10.1016/j.jaccas.2021.06.010. eCollection 2021 Oct 20. JACC Case Rep. 2021. PMID: 34729515 Free PMC article.
-
ST elevations in leads V1 to V5 may be caused by right coronary artery occlusion and acute right ventricular infarction.Am J Cardiol. 1984 Apr 1;53(8):991-6. doi: 10.1016/0002-9149(84)90623-4. Am J Cardiol. 1984. PMID: 6702712
-
Pathophysiology and ECG patterns of isolated right ventricular infarction with nondominant right coronary artery.J Cardiovasc Med (Hagerstown). 2013 Oct;14(10):740-4. doi: 10.2459/JCM.0b013e32835853a3. J Cardiovasc Med (Hagerstown). 2013. PMID: 22914309 Review.
-
Ventricular septal rupture with right ventricular wall dissection after inferior ventricular infarction: A case report and literature review.J Clin Ultrasound. 2019 May;47(4):247-252. doi: 10.1002/jcu.22684. Epub 2019 Jan 4. J Clin Ultrasound. 2019. PMID: 30614010 Review.
Cited by
-
Left ventricular free wall rupture caused by myocardial ischemia without treatable atherosclerotic coronary disease: a case series.J Cardiothorac Surg. 2024 Apr 12;19(1):202. doi: 10.1186/s13019-024-02690-2. J Cardiothorac Surg. 2024. PMID: 38609970 Free PMC article.
References
-
- Steg P.G., Goldberg R.J., Gore J.M., Fox K.A., Eagle K.A., Flather M.D., Sadiq I., Kasper R., Rushton-Mellor S.K., Anderson F.A., Investigators G.R.A.C.E. Baseline characteristics, management practices, and in-hospital outcomes of patients hospitalized with acute coronary syndromes in the Global Registry of Acute Coronary Events (GRACE) Am J Cardiol. 2002;90:358–363. - PubMed
-
- Becker R.C., Gore J.M., Lambrew C., Weaver W.D., Rubison R.M., French W.J., Tiefenbrunn A.J., Bowlby L.J., Rogers W.J. A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. J Am Coll Cardiol. 1996;27:1321–1326. - PubMed
-
- Setaro J.F., Cabin H.S. Right ventricular infarction. Cardiol Clin. 1992;10:69–90. - PubMed
-
- Cabin H.S., Clubb K.S., Wackers F.J., Zaret B.L. Right ventricular myocardial infarction with anterior wall left ventricular infarction: an autopsy study. Am Heart J. 1987;113:16–23. - PubMed
-
- Dzavik V., Sleeper L.A., Cocke T.P., Moscucci M., Saucedo J., Hosat S., Jiang X., Slater J., Lejemtel T., Hochman J.S., SHOCK Investigators Early revascularization is associated with improved survival in elderly patients with acute myocardial infarction complicated by cardiogenic shock: a report from the SHOCK Trial Registry. Eur Heart J. 2003;24:828–837. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
