

Evaluation of time to death after admission to an intensive care unit and factors associated with mortality: A retrospective longitudinal study
- PMID: 36506928
- PMCID: PMC9728075
- DOI: 10.4103/ijciis.ijciis_98_21
Evaluation of time to death after admission to an intensive care unit and factors associated with mortality: A retrospective longitudinal study
Abstract
Background: Among nonsurvivors admitted to the intensive care unit (ICU), some present early mortality while other patients, despite having a favorable evolution regarding the initial disease, die later due to complications related to hospitalization. This study aims to identify factors associated with the time until death after admission to an ICU of a university hospital.
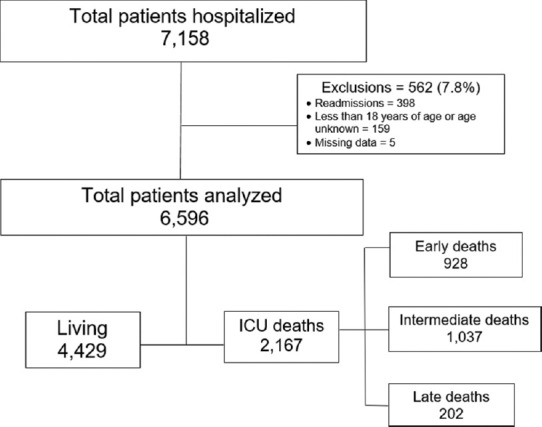
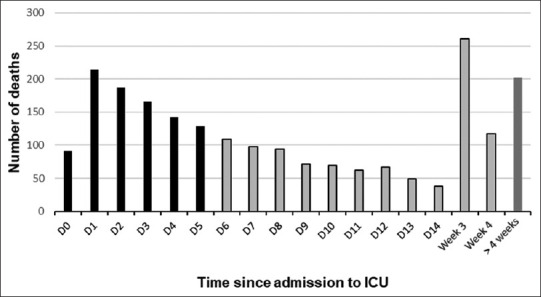
Methods: Retrospective longitudinal study that included adult patients admitted to the ICU between January 1, 2008, and December 31, 2017. Nonsurviving patients were divided into groups according to the length of time from admission to the ICU until death: Early (0-5 days), intermediate (6-28 days), and late (>28 days). Patients were considered septic if they had this diagnosis on admission to the ICU. Simple linear regression analysis was performed to evaluate the association between time to death over the years of the study. Multivariate cox regression was used to assess risk factors for the outcome in the ICU.
Results: In total, 6596 patients were analyzed. Mortality rate was 32.9% in the ICU. Most deaths occurred in the early (42.8%) and intermediate periods (47.9%). Patients with three or more dysfunctions on admission were more likely to die early (P < 0.001). The diagnosis of sepsis was associated with a higher mortality rate. The multivariate analysis identified age >60 years (hazard ratio [HR] 1.009), male (HR 1.192), mechanical ventilation (HR 1.476), dialysis (HR 2.297), and sequential organ failure assessment >6 (HR 1.319) as risk factors for mortality.
Conclusion: We found a higher proportion of early and intermediate deaths in the study period. The presence of three or more organ dysfunctions at ICU admission was associated with early death. The diagnosis of sepsis evident on ICU admission was associated with higher mortality.
Keywords: Intensive care units; in-hospital mortality; multiple organ failure; university hospitals.
Copyright: © 2022 International Journal of Critical Illness and Injury Science.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Brinkman S, Bakhshi-Raiez F, Abu-Hanna A, de Jonge E, de Keizer NF. Determinants of mortality after hospital discharge in ICU patients: Literature review and Dutch cohort study. Crit Care Med. 2013;41:1237–51. - PubMed
-
- Ziesmann MT, Marshall JC. Multiple organ dysfunction: The defining syndrome of sepsis. Surg Infect (Larchmt) 2018;19:184–90. - PubMed
LinkOut - more resources
Full Text Sources