

Neurocognitive Function Changes Following Kidney Transplant: A Prospective Study
- PMID: 36507052
- PMCID: PMC9732409
- DOI: 10.1016/j.xkme.2022.100560
Neurocognitive Function Changes Following Kidney Transplant: A Prospective Study
Abstract
Rationale & objective: Patients with advanced kidney disease are at risk for cognitive impairment, which may persist after kidney transplantation. We sought to understand changes in neurocognitive function domains utilizing comprehensive cognitive assessments.
Study design: Prospective cohort study.
Setting & population: Single-center study of patients undergoing kidney transplantation.
Exposure: Kidney transplantation.
Outcomes: Changes in neurocognitive function as measured by the Repeatable Battery for Assessment of Neuropsychological Status (RBANS) and the Trail Making Test Parts A and B (TRAIL A and B) before transplantation (baseline) and compared to 3 months and 12 months posttransplant.
Analytical approach: Wilcoxon signed-rank and linear mixed effect models were utilized to assess changes in neurocognitive scores at 3 months and 12 months compared to baseline.
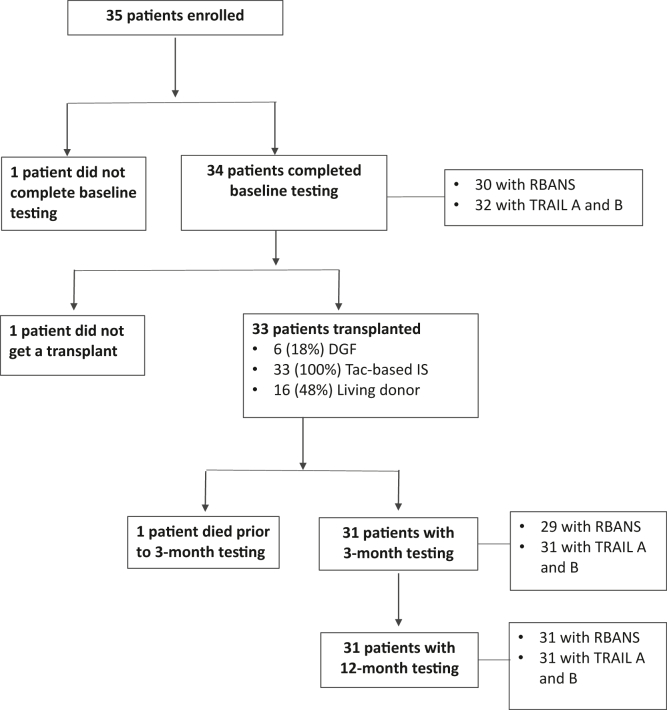
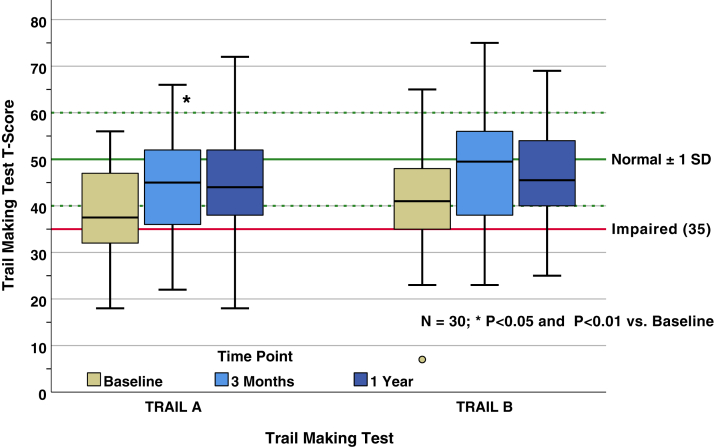
Results: Thirty-two patients were included with a mean age of 45 years, 47% female, 85% White, and 62% with at least some college education. Hypertension and diabetes were etiologies of kidney disease in 31% and 25% of patients, respectively. Baseline RBANS and TRAIL A and B scores averaged 84.7 ± 14, 40.4 ± 9.9, and 41 ± 11.5, respectively. Although there were posttransplant improvements in immediate and delayed memory at 3 months, these were not sustained at 12 months. There were no significant differences from baseline at 3 months and 12 months in RBANS index scores for language, visuospatial/constructional abilities, and attention. Compared to baseline, TRAIL A scores were not significantly different at 3 months but were significantly improved at 12 months, whereas TRAIL B scores improved significantly at both 3 months and 12 months.
Limitations: Single-center design and small sample size.
Conclusions: Utilizing comprehensive cognitive assessments, we found improvements in attention and executive function in the first posttransplant year as measured by TRAIL A and B. However, there was no significant change in global cognition as measured by RBANS. These findings identify cognitive domains for potential intervention in the posttransplant population.
Keywords: Kidney transplant; RBANS; TRAIL A; TRAIL B; neurocognitive function.
© 2022 The Authors.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
