

Detection of prostate cancer bone metastases with fast whole-body 99mTc-HMDP SPECT/CT using a general-purpose CZT system
- PMID: 36508016
- PMCID: PMC9743860
- DOI: 10.1186/s40658-022-00517-4
Detection of prostate cancer bone metastases with fast whole-body 99mTc-HMDP SPECT/CT using a general-purpose CZT system
Abstract
Background: We evaluated the effects of acquisition time, energy window width, and matrix size on the image quality, quantitation, and diagnostic performance of whole-body 99mTc-HMDP SPECT/CT in the primary metastasis staging of prostate cancer.
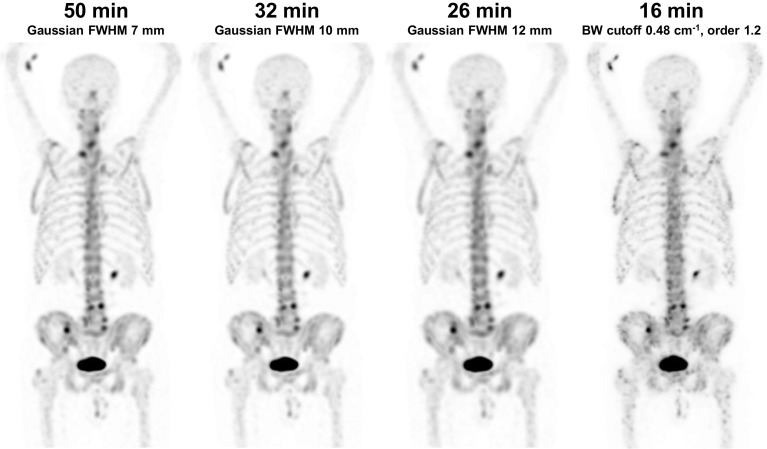
Methods: Thirty prostate cancer patients underwent 99mTc-HMDP SPECT/CT from the top of the head to the mid-thigh using a Discovery NM/CT 670 CZT system with list-mode acquisition, 50-min acquisition time, 15% energy window width, and 128 × 128 matrix size. The acquired list-mode data were resampled to produce data sets with shorter acquisition times of 41, 38, 32, 26, 20, and 16 min, narrower energy windows of 10, 8, 6, and 4%, and a larger matrix size of 256 × 256. Images were qualitatively evaluated by three experienced nuclear medicine physicians and quantitatively evaluated by noise, lesion contrast and SUV measurements. Diagnostic performance was evaluated from the readings of two experienced nuclear medicine physicians in terms of patient-, region-, and lesion-level sensitivity and specificity.
Results: The originally acquired images had the best qualitative image quality and lowest noise. However, the acquisition time could be reduced to 38 min, the energy window narrowed to 8%, and the matrix size increased to 256 × 256 with still acceptable qualitative image quality. Lesion contrast and SUVs were not affected by changes in acquisition parameters. Acquisition time reduction had no effect on the diagnostic performance, as sensitivity, specificity, accuracy, and area under the receiver-operating characteristic curve were not significantly different between the 50-min and reduced acquisition time images. The average patient-level sensitivities of the two readers were 88, 92, 100, and 96% for the 50-, 32-, 26-, and 16-min images, respectively, and the corresponding specificities were 78, 84, 84, and 78%. The average region-level sensitivities of the two readers were 55, 58, 59, and 56% for the 50-, 32-, 26-, and 16-min images, respectively, and the corresponding specificities were 95, 98, 96, and 95%. The number of equivocal lesions tended to increase as the acquisition time decreased.
Conclusion: Whole-body 99mTc-HMDP SPECT/CT can be acquired using a general-purpose CZT system in less than 20 min without any loss in diagnostic performance in metastasis staging of high-risk prostate cancer patients.
Keywords: Bone; CZT; SPECT/CT; Time reduction; Whole-body.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no potential competing of interest.
Figures

References
-
- Jambor I, Kuisma A, Ramadan S, Huovinen R, Sandell M, Kajander S, et al. Prospective evaluation of planar bone scintigraphy, SPECT, SPECT/CT, 18F-NaF PET/CT and whole body 1.5T MRI, including DWI, for the detection of bone metastases in high risk breast and prostate cancer patients: SKELETA clinical trial. Acta Oncol. 2016;55:59–67. doi: 10.3109/0284186X.2015.1027411. - DOI - PubMed
-
- Bartel TB, Kuruva M, Gnanasegaran G, Cohen EJ, Weissman AF, Yarbrough TL. SNMMI procedure standard for bone scintigraphy 4.0. J Nucl Med Technol. 2018;46:398–404. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
