

Low incidence of advanced neurological burden but high incidence of age-related conditions that are dementia risk factors in aging people living with HIV: a data-linkage 10-year follow-up study
- PMID: 36508059
- PMCID: PMC10185650
- DOI: 10.1007/s13365-022-01104-0
Low incidence of advanced neurological burden but high incidence of age-related conditions that are dementia risk factors in aging people living with HIV: a data-linkage 10-year follow-up study
Abstract
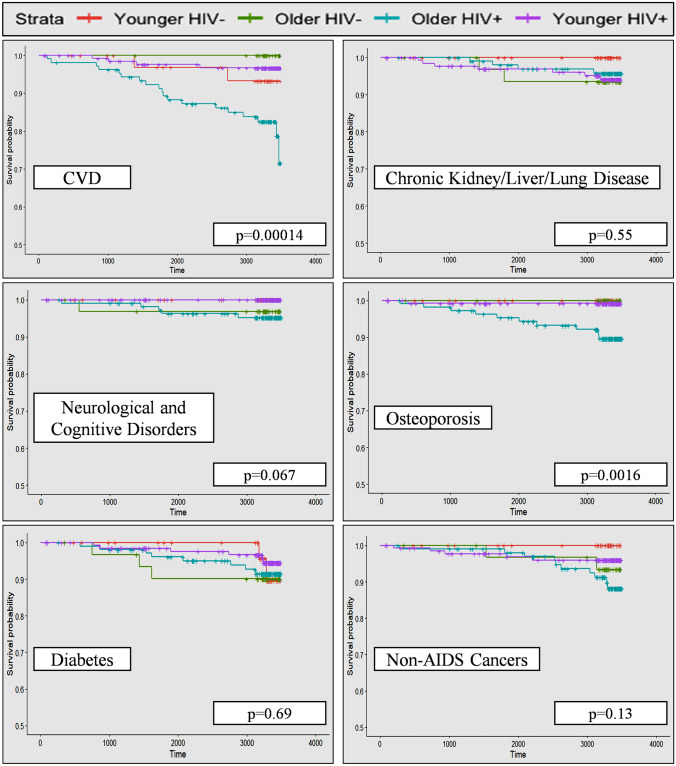
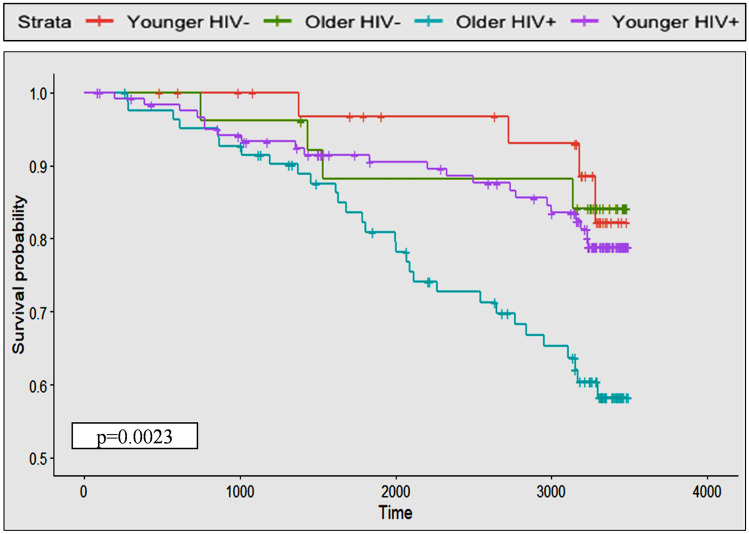
Although increasing research is focusing on age-related comorbidities (ARC) among people living with HIV (PLHIV), no studies have concomitantly assessed non-HIV age-related neurological disorders (e.g., Alzheimer's dementia). A total of 254 PLHIV and 69 HIV-negative controls completed baseline medical history and cognitive testing. ARC data were collected from medical records over the subsequent 9-10 years and included all types of strokes, all types of dementia, mild cognitive impairment, Parkinson's disease, motor neuron disease (grouped into a non-HIV age-related neurological category), cardiovascular disease, chronic kidney disease, chronic liver disease, chronic lung disease, non-AIDS cancers, osteoporosis, and diabetes. Kaplan-Meier curves assessed differences in the incident rates (per 1000 person year) of groups of ARC as defined above and combined ARC (i.e., development of any of the ARC) among younger (baseline age < 50) and older (baseline age ≥ 50) PLHIV and younger and older controls. Cox-proportional hazard models assessed the individual and interaction effects of HIV status and chronological age, in addition to a range of demographic and clinical variables including historical and baseline HIV brain involvement on the risk of developing combined ARC. Older PLHIV had a higher incidence of cardiovascular disease, osteoporosis, and combined ARC compared to other groups (p < 0.05). Incident rate of non-HIV age-related neurological disorders was 2.3 [0.93, 4.79] per 1000 person year. While this incident rate was higher in older PLHIV (5.37 [1.97, 11.92]) than older HIV-negative participants (3.58 [0.18-17.67]), this was not significant. In multivariate analyses, HIV status and chronological age, but not their interaction, and smoking were associated with higher risk of combined ARC (p < 0.05). In analyses focusing on PLHIV, older age and taking abacavir/efavirenz/atazanavir/darunavir containing antiretroviral treatments at the time of diagnosis were associated with greater ARC (p < 0.05). Non-HIV age-related neurological disorders are uncommon in older PLHIV, where the majority were < 70 years of age at the end of follow-up. However, the greater burden of ARC among older PLHIV, most of which are established dementia risk factors, warrants the establishment of commensurate prevention strategies and greater attention to neurocognitive screening.
Keywords: Aging; Comorbidities; HIV; Incidence; Neurological disorders.
© 2022. The Author(s).
Conflict of interest statement
Bruce J. Brew received speaker honorarium from Janssen. Mark Bloch received funds for medical advisory boards and educational meetings from Gilead Sciences, Abbvie, Janssen, and ViiV Healthcare. He also received funding for research from Gilead Sciences, ViiV Healthcare, MSD, Abbvie, and GSK. All the other authors declare no conflict of interests.
Figures
References
-
- Aung HL, Gates TM, Mao L, Brew BJ, Rourke SB, Cysique LA (2022) Abnormal cognitive aging in people with HIV: evidence from Data Integration between two countries’ cohort studies. AIDS 10:1097 - PubMed
-
- Aung HL, Kootar S, Gates TM, Brew BJ, Cysique LA. How all-type dementia risk factors and modifiable risk interventions may be relevant to the first-generation aging with HIV infection? Eur Geriatr Med. 2019;10:227–238. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
