

Neural Drive Impairment in Chronic Kidney Disease Patients Is Associated with Neuromuscular Fatigability and Fatigue
- PMID: 36508212
- PMCID: PMC9997639
- DOI: 10.1249/MSS.0000000000003090
Neural Drive Impairment in Chronic Kidney Disease Patients Is Associated with Neuromuscular Fatigability and Fatigue
Abstract
Introduction: Chronic kidney disease (CKD) patients have a high degree of fatigue relating to neuromuscular symptoms. There is a lack of evidence regarding the etiology of neuromuscular fatigability in elderly CKD patients.
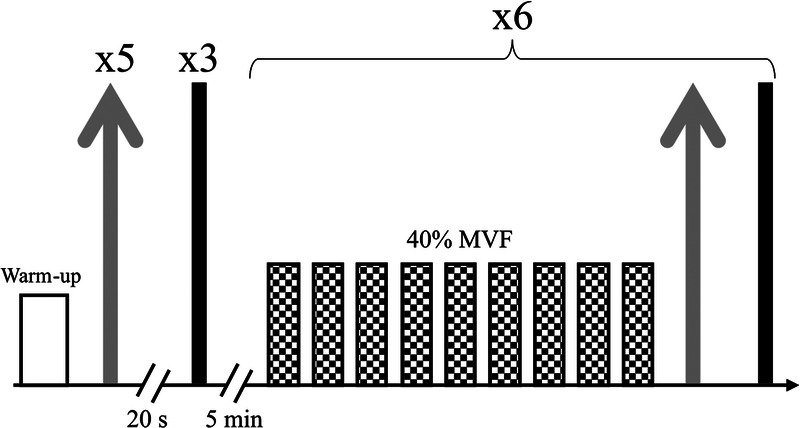
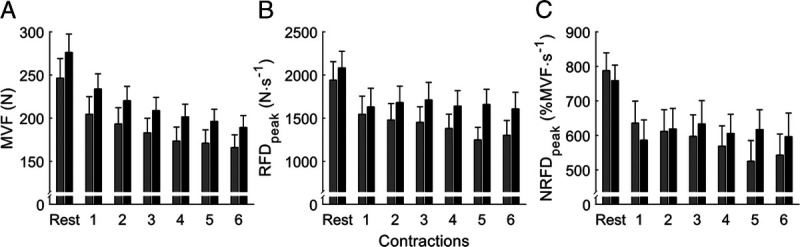
Methods: Inclusion criteria are as follows: age ≥60 yr, glomerular filtration rate (GFR) <45 mL·min -1 per 1.73 m 2 in CKD patients, and GFR >60 mL·min -1 ·1.73 m -2 in controls. The fatigability protocol consisted in a submaximal handgrip task at 40% peak force. Fatigue was assessed using the Multidimensional Fatigue Inventory-20 items (MFI-20) and the Functional Assessment of Chronic Illness Therapy-Fatigue questionnaires. Peak rate of force development (RFD peak , normalized: NRFD peak ) and rate of EMG rise (RER) were measured during explosive contractions; peak force and mean surface EMG were measured during maximum voluntary contractions. Multilevel models tested neuromuscular parameters adjusted for clinical and Multidimensional Fatigue Inventory-20 items subscales. Neuromuscular fatigability contribution to fatigue description was tested using model comparison.
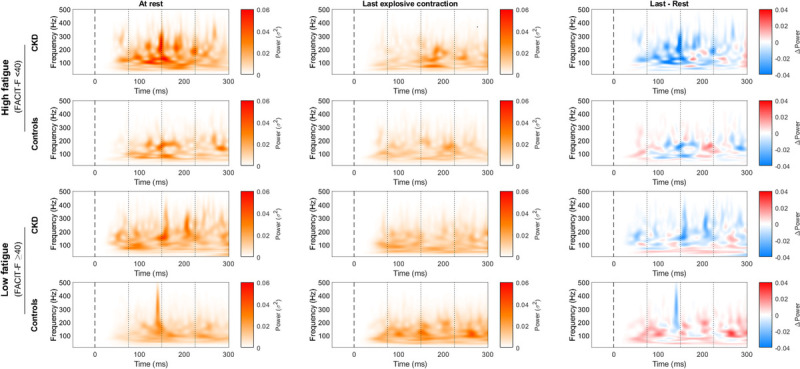
Results: The study included 102 participants; 45 CKD patients and 57 controls. CKD mainly affected the mental and the reduced motivation subscales of fatigue. CKD was associated with greater neuromuscular fatigability assessed using NRFD peak (group-time interaction, -16.7 % MVF·s -1 , P = 0.024), which increased with fatigue severity ( P = 0.018) and with a higher rate of decrement in RER compared with controls (RER at 50 ms: β = -121.2 μV·s -1 , P = 0.016, and β = -48.5 μV·s -1 , P = 0.196, respectively). Furthermore, these patients show an association between the reduced motivation subscale and the RER (e.g., 30 ms: β = -59.8% EMG peak ·s -1 , P < 0.001). Only peak force fatigability contributed to fatigue variance, whereas RFD peak did not.
Conclusions: In CKD patients, the neuromuscular fatigability assessed using RFD peak is related to an impairment in motor-unit recruitment or discharge rates, whereas only peak force fatigability was related to fatigue. This suggests that targeting exercise interventions might lessen fatigue and improve quality of life in CKD patients.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American College of Sports Medicine.
Figures
Similar articles
-
Analysis of the rate of force development reveals high neuromuscular fatigability in elderly patients with chronic kidney disease.J Cachexia Sarcopenia Muscle. 2023 Oct;14(5):2016-2028. doi: 10.1002/jcsm.13280. Epub 2023 Jul 13. J Cachexia Sarcopenia Muscle. 2023. PMID: 37439126 Free PMC article.
-
PhysIOpathology of NEuromuscular function rElated to fatigue in chronic Renal disease in the elderly (PIONEER): study protocol.BMC Nephrol. 2020 Jul 25;21(1):305. doi: 10.1186/s12882-020-01976-6. BMC Nephrol. 2020. PMID: 32711479 Free PMC article.
-
Fatigability and the Role of Neuromuscular Impairments in Chronic Kidney Disease.Am J Nephrol. 2022;53(4):253-263. doi: 10.1159/000523714. Epub 2022 Mar 28. Am J Nephrol. 2022. PMID: 35344954 Free PMC article. Review.
-
Upper-Limb Muscle Fatigability in Para-Athletes Quantified as the Rate of Force Development in Rapid Contractions of Submaximal Amplitude.J Funct Morphol Kinesiol. 2024 Jun 20;9(2):108. doi: 10.3390/jfmk9020108. J Funct Morphol Kinesiol. 2024. PMID: 38921644 Free PMC article.
-
Rate of Force Development as an Indicator of Neuromuscular Fatigue: A Scoping Review.Front Hum Neurosci. 2021 Jul 9;15:701916. doi: 10.3389/fnhum.2021.701916. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34305557 Free PMC article.
Cited by
-
Exercise for patients with chronic kidney disease: from cells to systems to function.Am J Physiol Renal Physiol. 2024 Mar 1;326(3):F420-F437. doi: 10.1152/ajprenal.00302.2023. Epub 2024 Jan 11. Am J Physiol Renal Physiol. 2024. PMID: 38205546 Free PMC article. Review.
-
Hemodynamic and neuromuscular basis of reduced exercise capacity in patients with end-stage renal disease.Eur J Appl Physiol. 2024 Jul;124(7):1991-2004. doi: 10.1007/s00421-024-05427-0. Epub 2024 Feb 19. Eur J Appl Physiol. 2024. PMID: 38374473
-
Review of Exercise Interventions to Improve Clinical Outcomes in Nondialysis CKD.Kidney Int Rep. 2024 Aug 2;9(11):3097-3115. doi: 10.1016/j.ekir.2024.07.032. eCollection 2024 Nov. Kidney Int Rep. 2024. PMID: 39534200 Free PMC article. Review.
-
Measuring objective fatigability and autonomic dysfunction in clinical populations: How and why?Front Sports Act Living. 2023 Mar 30;5:1140833. doi: 10.3389/fspor.2023.1140833. eCollection 2023. Front Sports Act Living. 2023. PMID: 37065809 Free PMC article. Review.
-
Quality matters: chronic kidney disease progression is associated with reduced muscle strength independently of changes in skeletal muscle mass: an observational study.Clin Kidney J. 2025 Feb 4;18(3):sfaf036. doi: 10.1093/ckj/sfaf036. eCollection 2025 Mar. Clin Kidney J. 2025. PMID: 40052163 Free PMC article.
References
-
- Artom M, Moss-Morris R, Caskey F, Chilcot J. Fatigue in advanced kidney disease. Kidney Int. 2014;86(3):497–505. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
