

Factors Associated With Quality Care Among Adults With Rheumatoid Arthritis
- PMID: 36508216
- PMCID: PMC9856345
- DOI: 10.1001/jamanetworkopen.2022.46299
Factors Associated With Quality Care Among Adults With Rheumatoid Arthritis
Abstract
Importance: Although quality care markers exist for patients with rheumatoid arthritis (RA), the predictors of meeting these markers are unclear.
Objective: To explore factors associated with quality care among patients with RA.
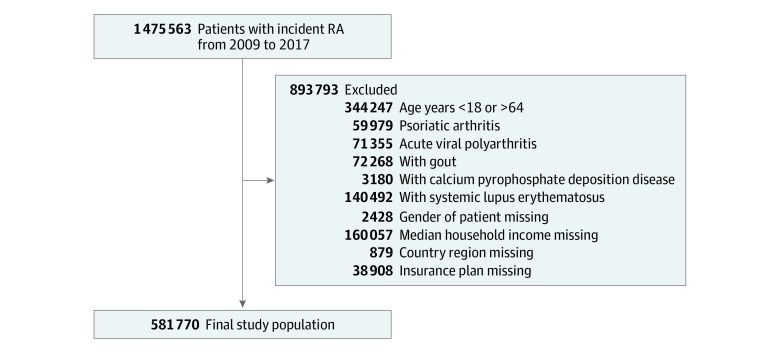
Design, setting, and participants: A retrospective cohort study using insurance claims from 2009 to 2017 was conducted, and 6 sequential logistic regression models were built to evaluate quality care markers. Quality care markers were measured at 1 year post-RA diagnosis for each patient. The MarketScan Research Database, which contains commercial and Medicare Advantage administrative claims data from more than 100 million individuals in the US, was used to identify patients aged 18 to 64 years with a diagnosis claim for RA. Patients with conditions presenting similar to RA and missing demographic characteristics were excluded. Data analysis occurred between February 18 and May 5, 2022.
Exposures: Success or failure to meet selected RA quality care markers within 1 year after RA diagnosis.
Main outcomes and measures: Prevalence of meeting successive quality care markers for RA.
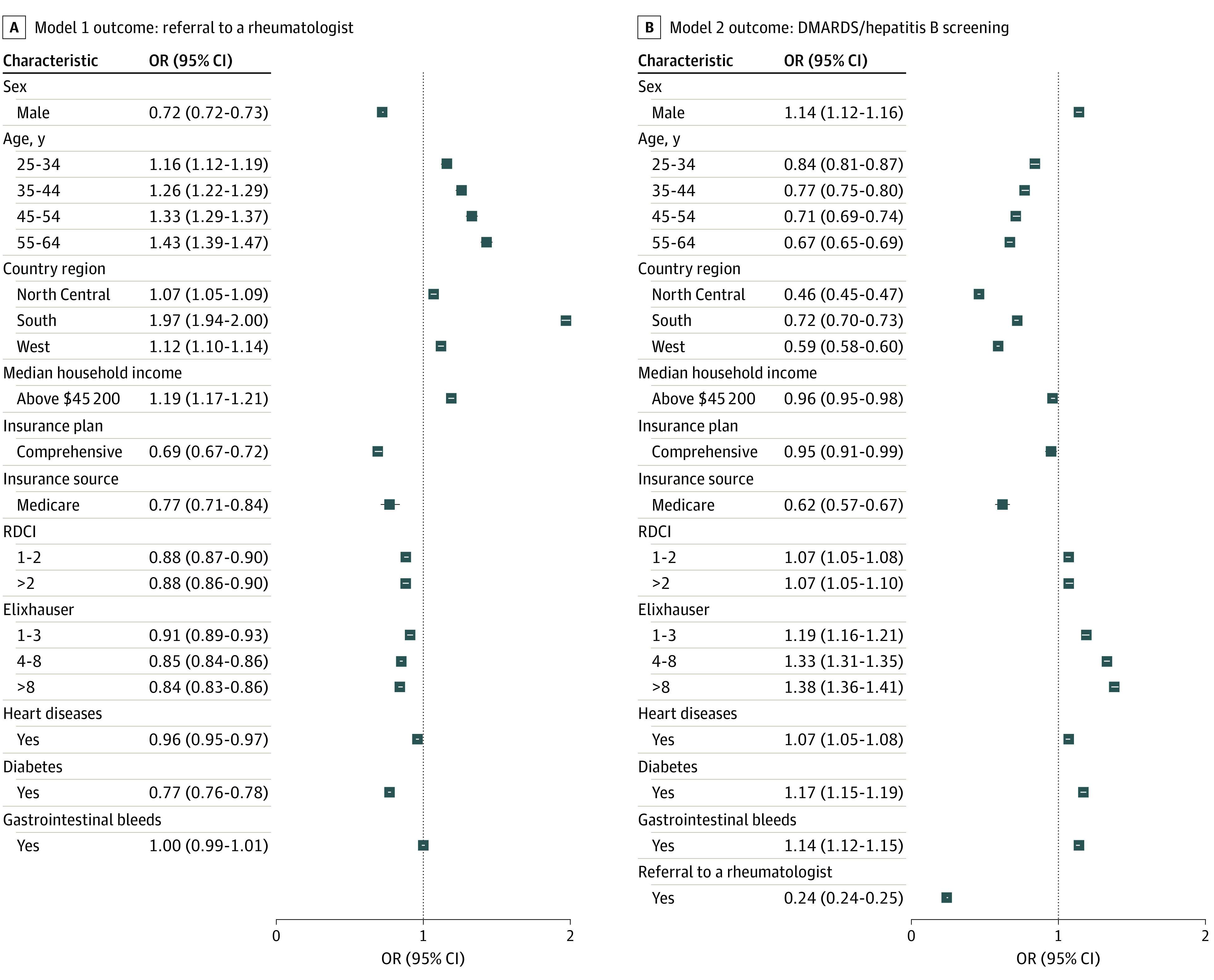
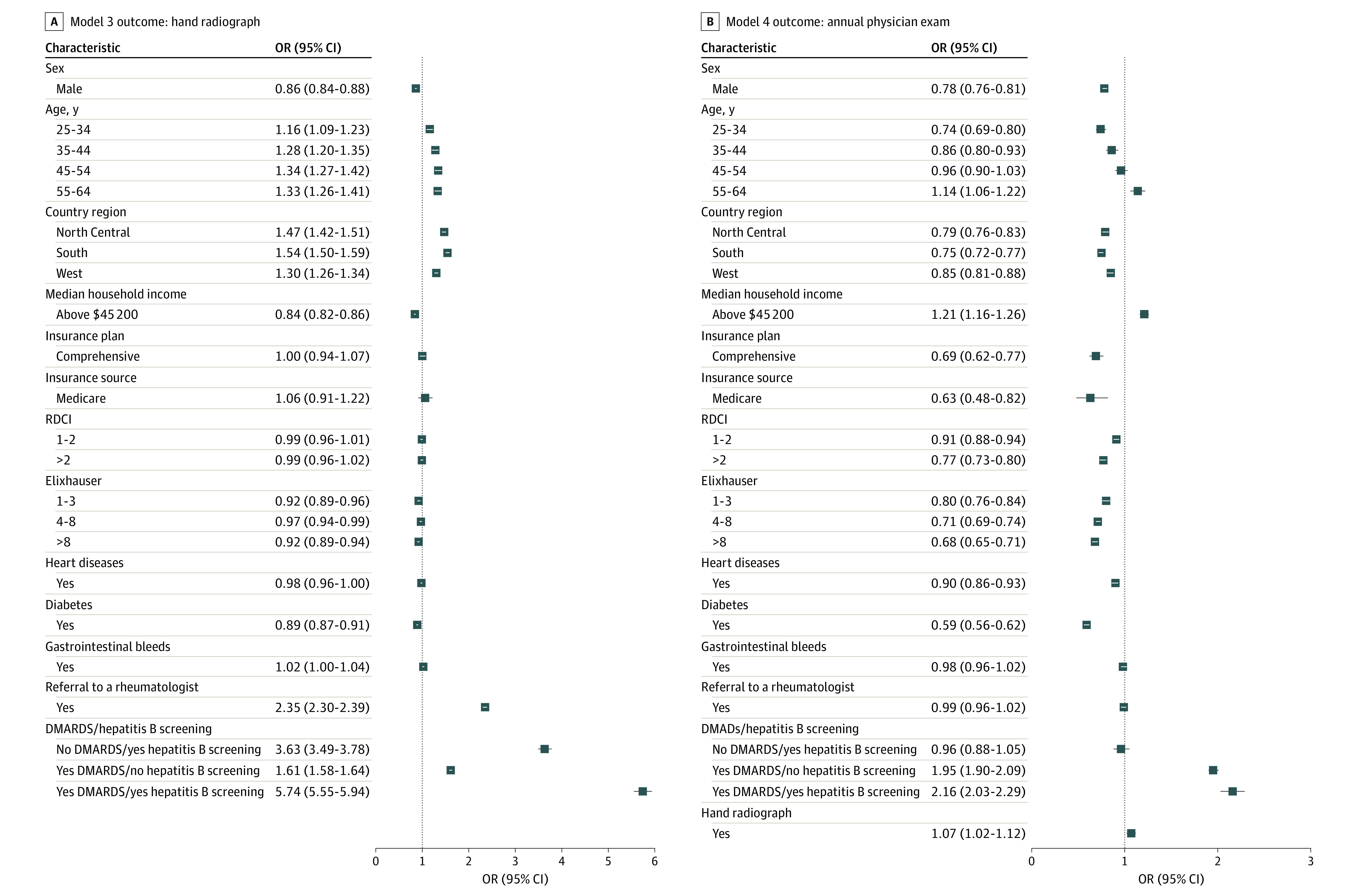
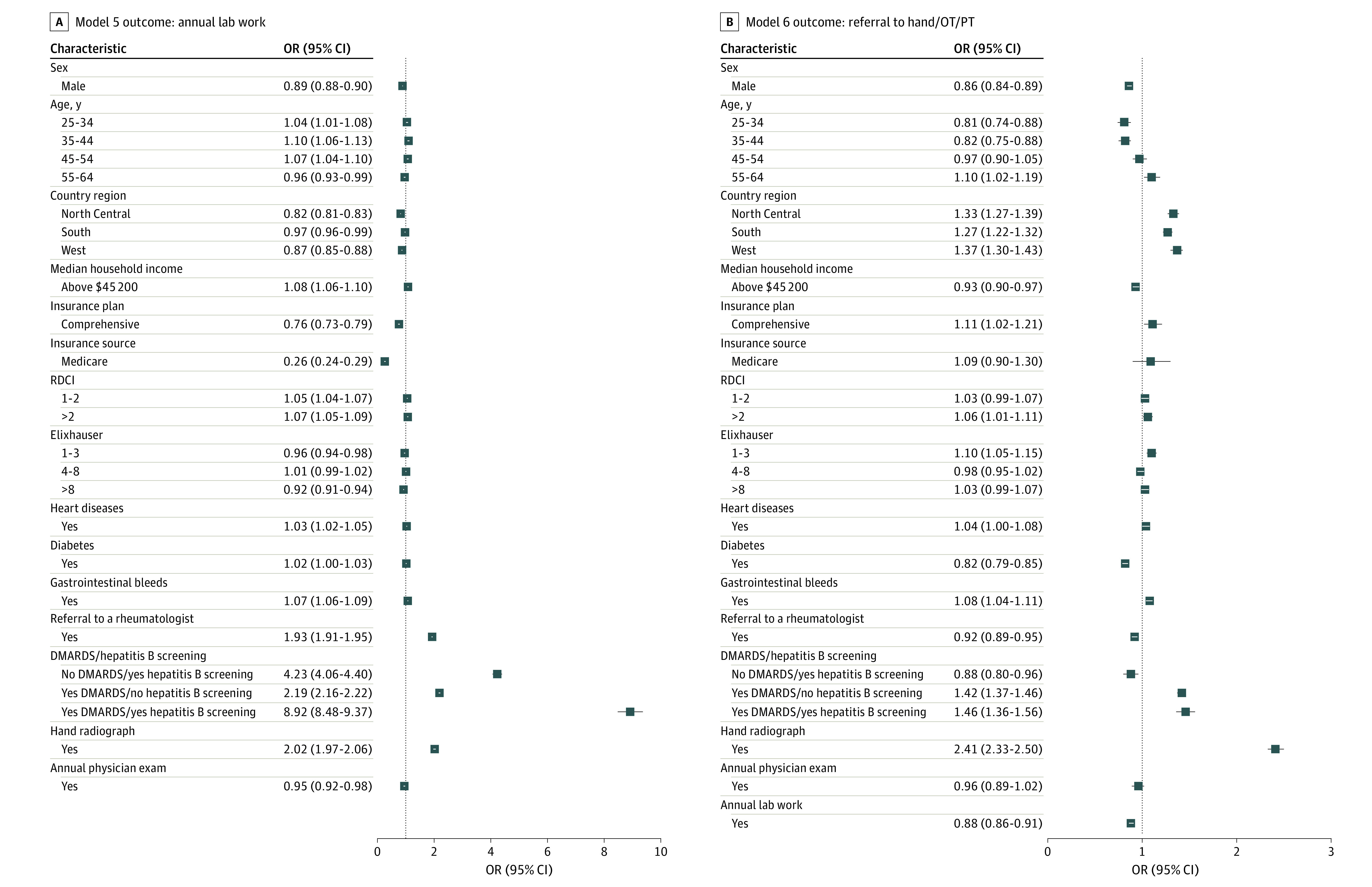
Results: Among 581 770 patients, 430 843 (74.1%) were women and the mean (SD) age was 48.9 (11.3) years. Most patients (236 285 [40.6%]) resided in the South and had an income less than or equal to $45 200 (490 366 [84.3%]). Of the total study population, 399 862 individuals (68.7%) met at least 1 quality care marker and 181 908 (31.3%) met 0 markers. Most commonly, patients met annual laboratory testing (299 323 [51.5%]) and referral to a rheumatologist (256 765 [44.1%]) markers. The least met marker was receiving hepatitis B screening prior to initiation of disease-modifying antirheumatic drug (DMARD) therapy (18 548 [3.2%]). Women were most likely to meet all quality care markers except receiving DMARDs with hepatitis B screening (odds ratio, 1.14; 95% CI, 1.12-1.16). Individuals with lower median household income had lower odds of receiving a rheumatologist referral, an annual physical examination, or annual laboratory testing, but greater odds of receiving the other quality care markers. Patients with Medicare and those with comorbidities were generally less likely to meet quality care markers.
Conclusions and relevance: In this cohort study of patients with RA, findings indicated downstream associations with rheumatologist referral and receiving DMARDs and varied associations between meeting quality care markers and patient characteristics. These findings suggest that prioritizing early care, especially for vulnerable patients, will ensure that quality care continues.
Conflict of interest statement
Figures
References
-
- Saag KG, Yazdany J, Alexander C, et al. ; American College of Rheumatology Quality Measurement White Paper Development Workgroup . Defining quality of care in rheumatology: the American College of Rheumatology white paper on quality measurement. Arthritis Care Res (Hoboken). 2011;63(1):2-9. doi:10.1002/acr.20369 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
