

A prediction model for asthma exacerbations after stopping asthma biologics
- PMID: 36509405
- PMCID: PMC9992017
- DOI: 10.1016/j.anai.2022.11.025
A prediction model for asthma exacerbations after stopping asthma biologics
Abstract
Background: Little is known regarding the prediction of the risks of asthma exacerbation after stopping asthma biologics.
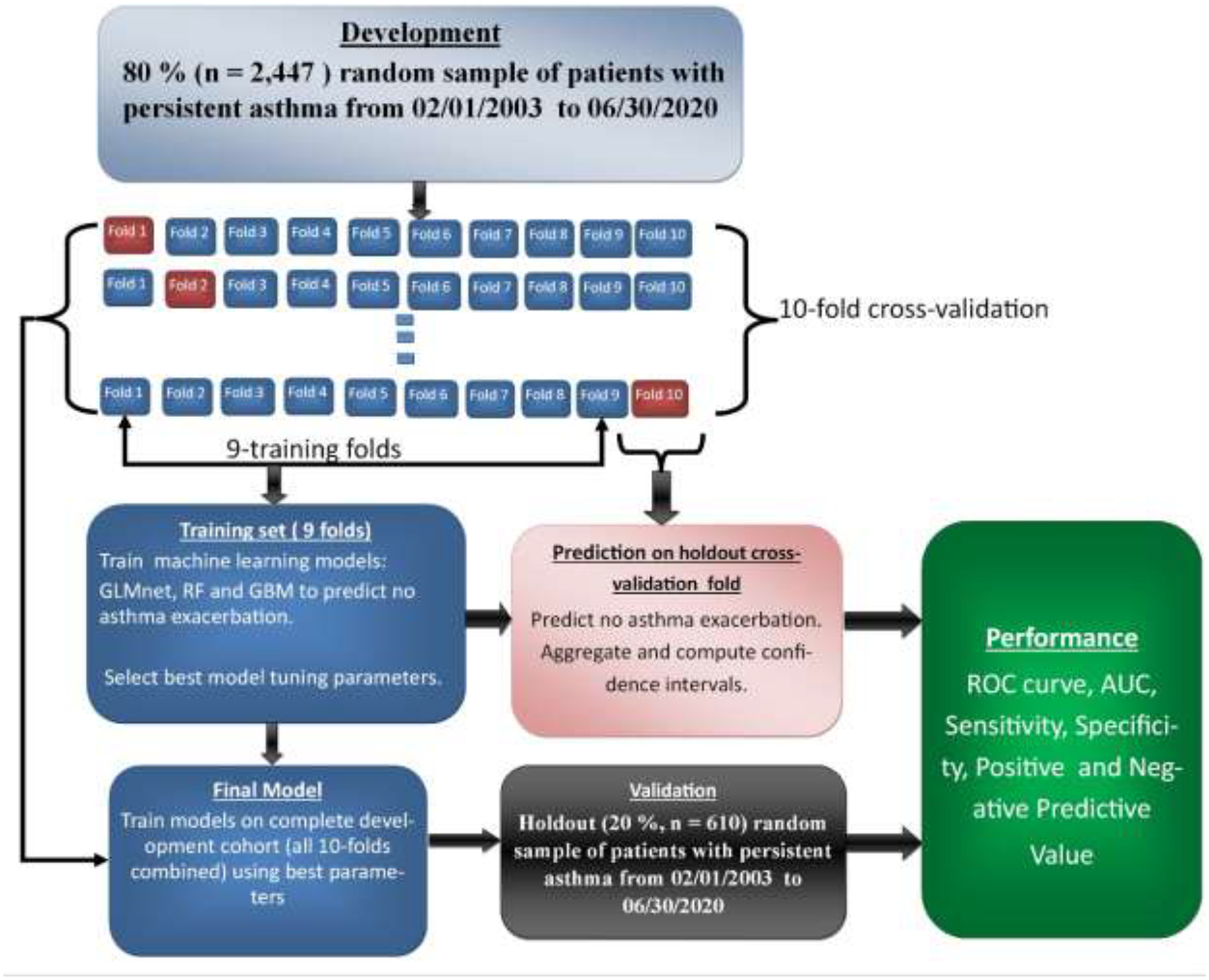
Objective: To develop and validate a predictive model for the risk of asthma exacerbations after stopping asthma biologics using machine learning models.
Methods: We identified 3057 people with asthma who stopped asthma biologics in the OptumLabs Database Warehouse and considered a wide range of demographic and clinical risk factors to predict subsequent outcomes. The primary outcome used to assess success after stopping was having no exacerbations in the 6 months after stopping the biologic. Elastic-net logistic regression (GLMnet), random forest, and gradient boosting machine models were used with 10-fold cross-validation within a development (80%) cohort and validation cohort (20%).
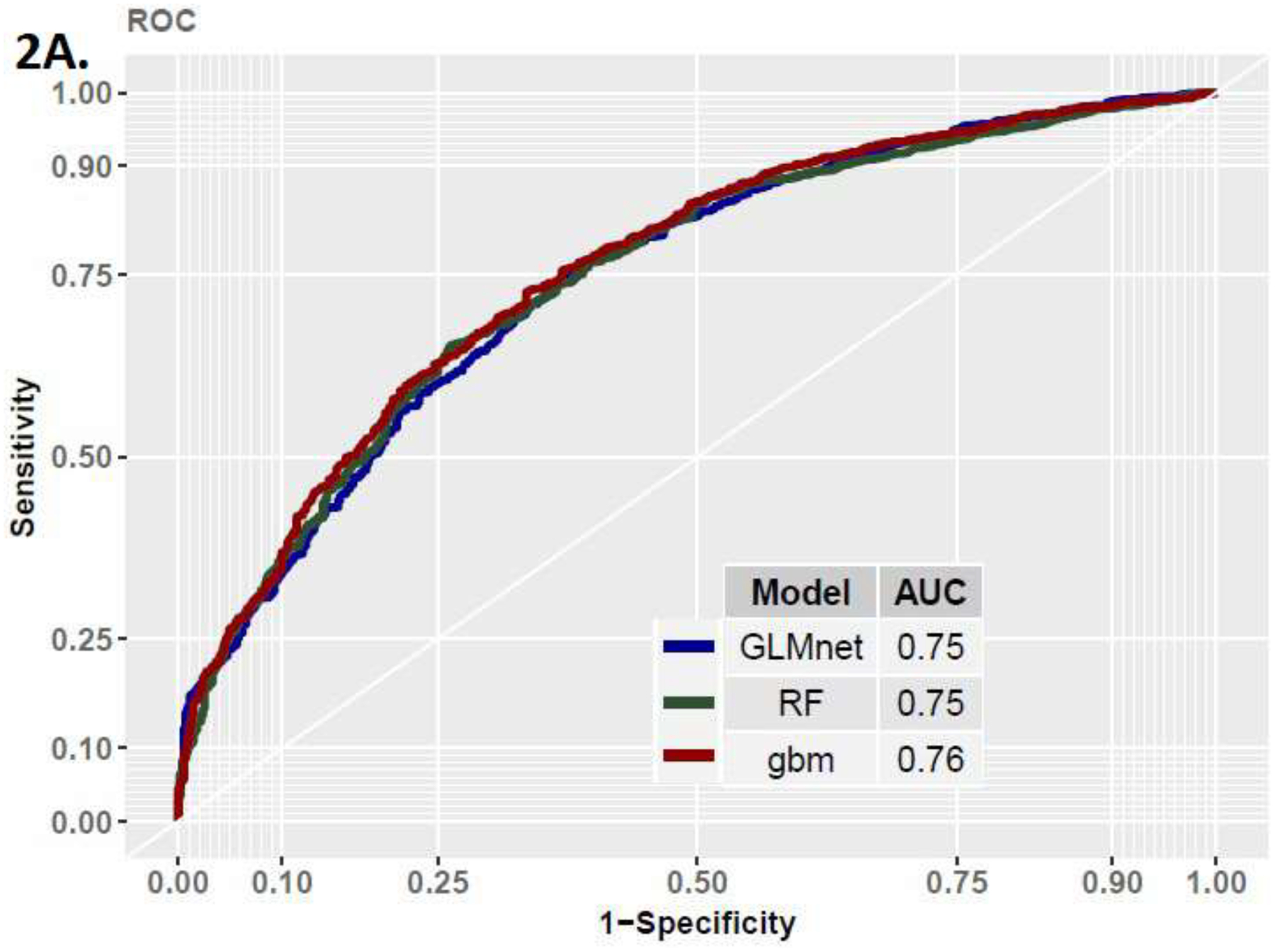
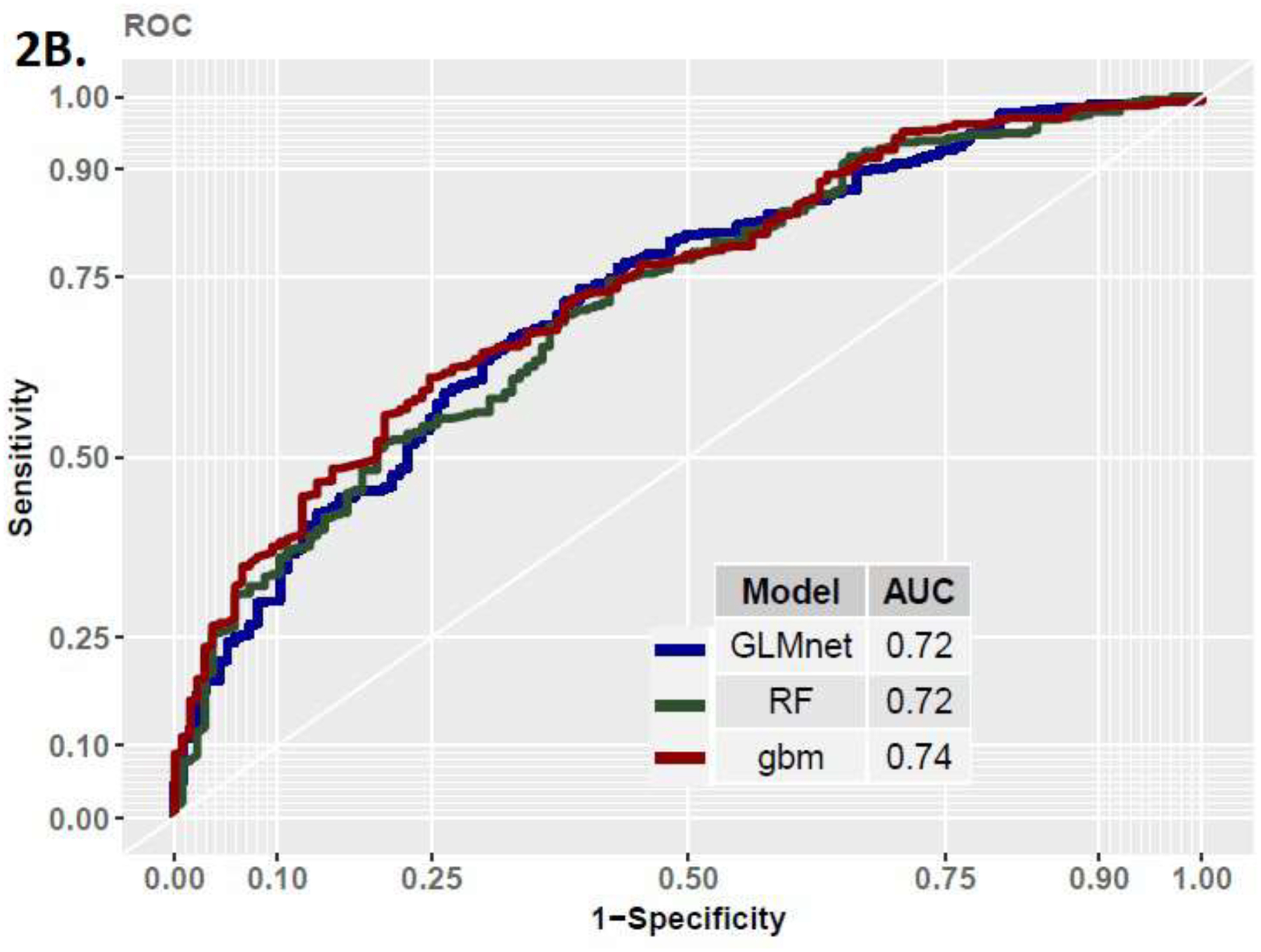
Results: The mean age of the total cohort was 47.1 (SD, 17.1) years, 1859 (60.8%) were women, 2261 (74.0%) were White, and 1475 (48.3%) were in the Southern region of the United States. The elastic-net logistic regression model yielded an area under the curve (AUC) of 0.75 (95% confidence interval [CI], 0.71-0.78) in the development and an AUC of 0.72 in the validation cohort. The random forest model yielded an AUC of 0.75 (95% CI, 0.68-0.79) in the development cohort and an AUC of 0.72 in the validation cohort. The gradient boosting machine model yielded an AUC of 0.76 (95% CI, 0.72-0.80) in the development cohort and an AUC of 0.74 in the validation cohort.
Conclusion: Outcomes after stopping asthma biologics can be predicted with moderate accuracy using machine learning methods.
Copyright © 2022 American College of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Gionfriddo MR, Hagan JB, Rank MA. Why and how to step down chronic asthma drugs. BMJ. 2017;359:j4438. - PubMed
-
- DiMango E, Rogers L, Reibman J, Gerald LB, Brown M, Sugar EA, et al. Risk factors for asthma exacerbation and treatment failure in adults and adolescents with well-controlled asthma during continuation and step-down therapy. Ann Am Thorac Soc. 2018; 15(8):955–961. - PubMed
-
- Perez de Llano L, Garcia-Rivero JL, Urrutia I, Martinez-Moragon E, Ramos J, Cebollero P, et al. A simple score for future risk prediction in patients with controlled asthma who undergo guidelines-based step-down strategy. J Allergy Clin Immunol Pract. 2019;7:1214–21. - PubMed
-
- Saito N, Kamata A, Itoga M, Tamaki M, Kayaba H, Ritz T. Assessment of biological, psychological and adherence factors in the prediction of step-down treatment for patients with well-controlled asthma. Clin Exp Allergy. 2017;(47):467–478. - PubMed
-
- Martinez-Moragon E, Delgado J, Mogrovejo S, Fernandez-Sanchez T, Jesus JL, Angel MOM, et al. Factors that determine the loss of control when reducing therapy by steps in the treatment of moderate-severe asthma in standard clinical practice: A multicentre Spanish study. Rev Clin Esp. 2020;220:86–93. - PubMed
