

Prospective multicentre study of host response signatures in neonatal sepsis in Sub Saharan Africa
- PMID: 36509812
- PMCID: PMC9743113
- DOI: 10.1038/s41598-022-25892-x
Prospective multicentre study of host response signatures in neonatal sepsis in Sub Saharan Africa
Abstract
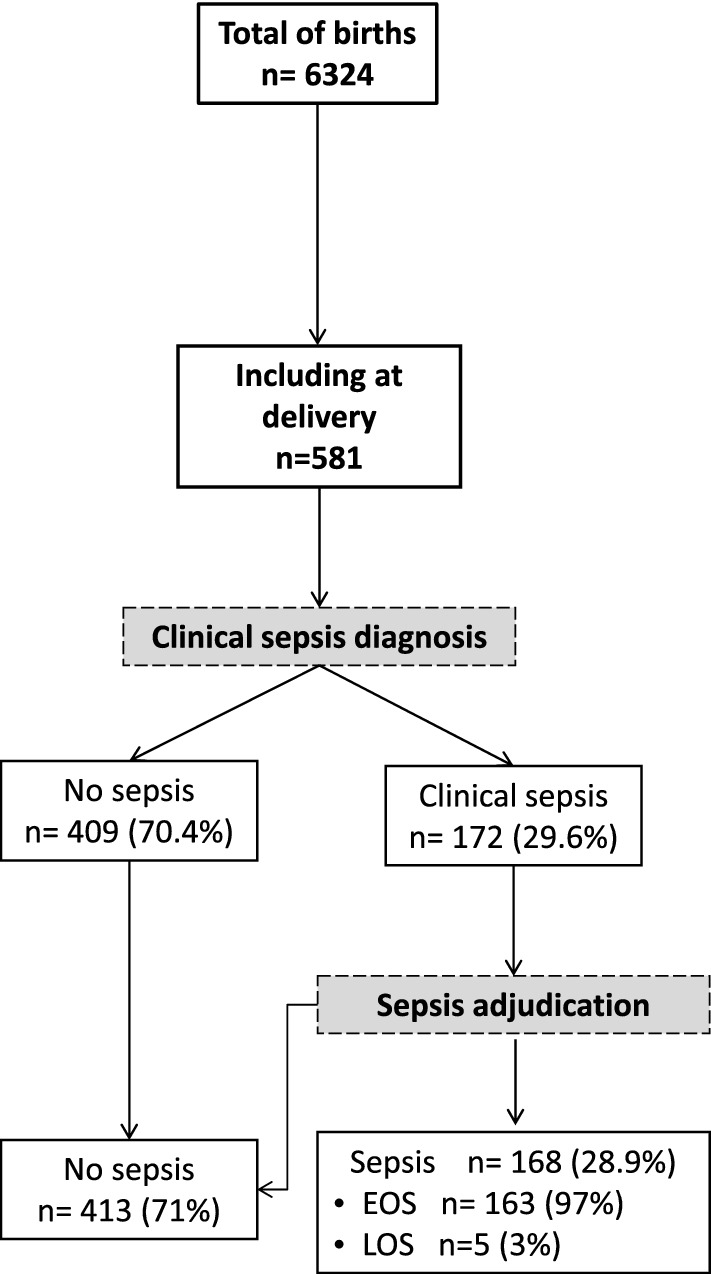
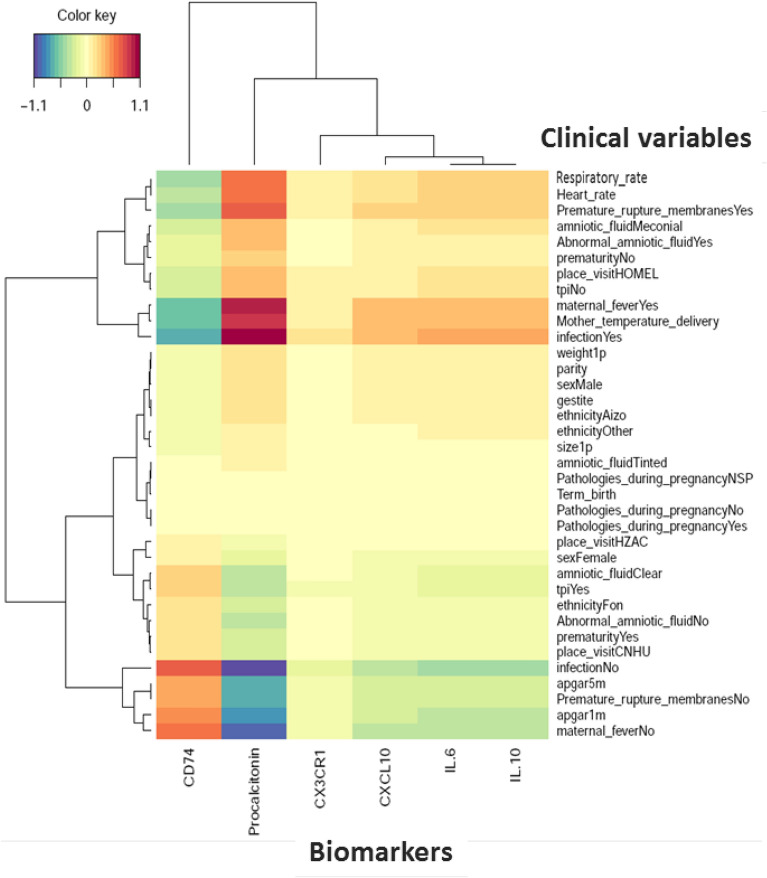
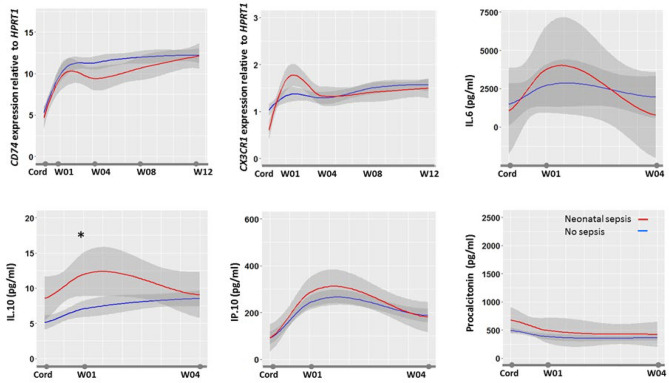
Few biomarkers for sepsis diagnosis are commonly used in neonatal sepsis. While the role of host response is increasingly recognized in sepsis pathogenesis and prognosis, there is a need for evaluating new biomarkers targeting host response in regions where sepsis burden is high and medico-economic resources are scarce. The objective of the study is to evaluate diagnostic and prognostic accuracy of biomarkers of neonatal sepsis in Sub Saharan Africa. This prospective multicentre study included newborn infants delivered in the Abomey-Calavi region in South Benin and their follow-up from birth to 3 months of age. Accuracy of transcriptional (CD74, CX3CR1), proteic (PCT, IL-6, IL-10, IP-10) biomarkers and clinical characteristics to diagnose and prognose neonatal sepsis were measured. At delivery, cord blood from all consecutive newborns were sampled and analysed, and infants were followed for a 12 weeks' period. Five hundred and eighty-one newborns were enrolled. One hundred and seventy-two newborns developed neonatal sepsis (29.6%) and death occurred in forty-nine infants (8.4%). Although PCT, IL-6 and IP-10 levels were independently associated with sepsis diagnosis, diagnostic accuracy of clinical variables combinations was similar to combinations with biomarkers and superior to biomarkers alone. Nonetheless, CD74, being the only biomarkers independently associated with mortality, showed elevated prognosis accuracy (AUC > 0.9) either alone or in combination with other biomarkers (eg. CD74/IP-10) or clinical criterion (eg. Apgar 1, birth weight). These results suggest that cord blood PCT had a low accuracy for diagnosing early onset neonatal sepsis in Sub Saharan African neonates, while association of clinical criterion showed to be more accurate than any biomarkers taken independently. At birth, CD74, either associated with IP-10 or clinical criterion, had the best accuracy in prognosing sepsis mortality.Trial registration Clinicaltrial.gov registration number: NCT03780712. Registered 19 December 2018. Retrospectively registered.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- IHME. Global Burden of Disease Collaborative Network. (2018).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
