

Pseudomonas aeruginosa aggregation and Psl expression in sputum is associated with antibiotic eradication failure in children with cystic fibrosis
- PMID: 36509824
- PMCID: PMC9744911
- DOI: 10.1038/s41598-022-25889-6
Pseudomonas aeruginosa aggregation and Psl expression in sputum is associated with antibiotic eradication failure in children with cystic fibrosis
Abstract
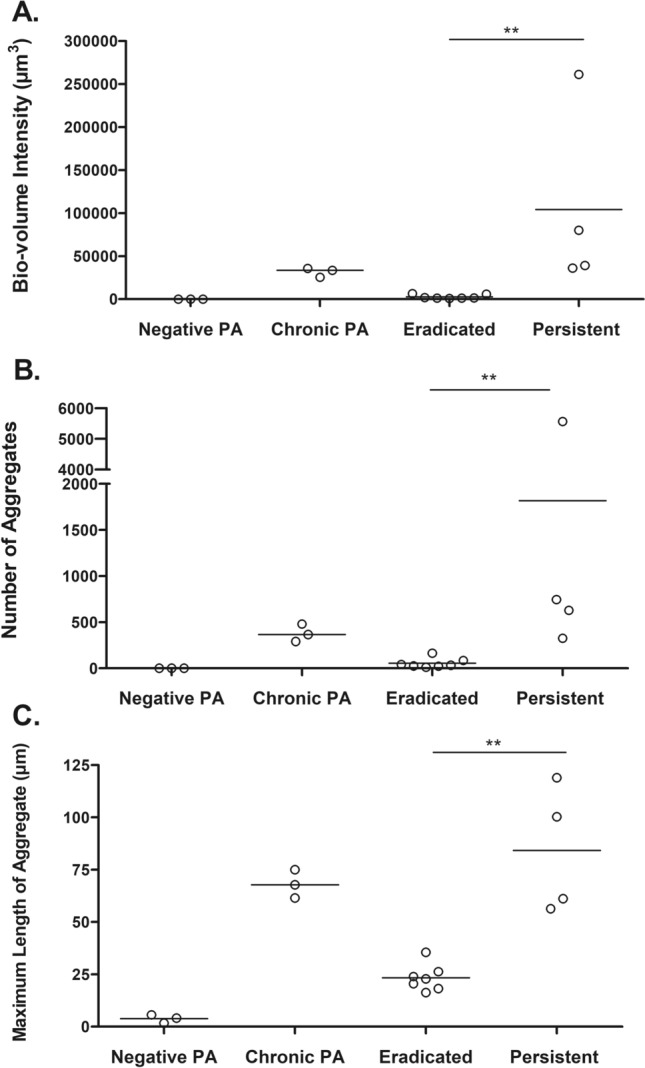
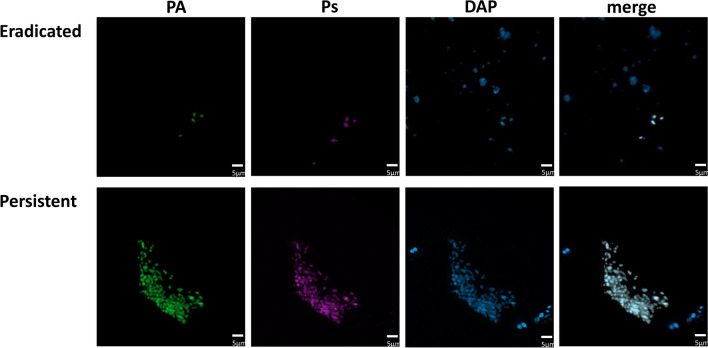
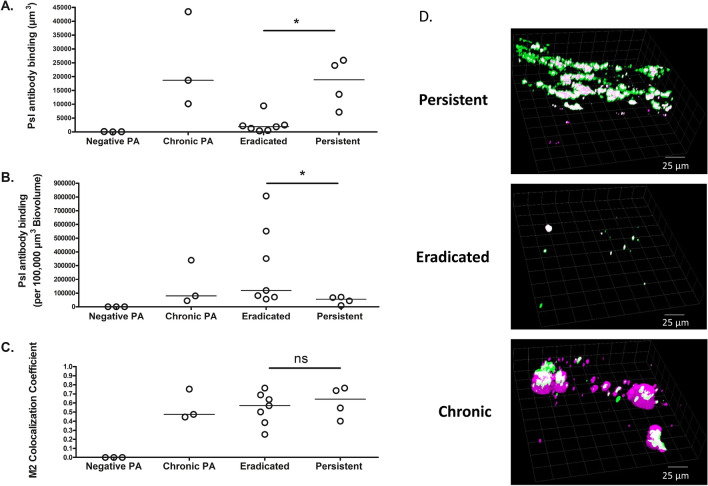
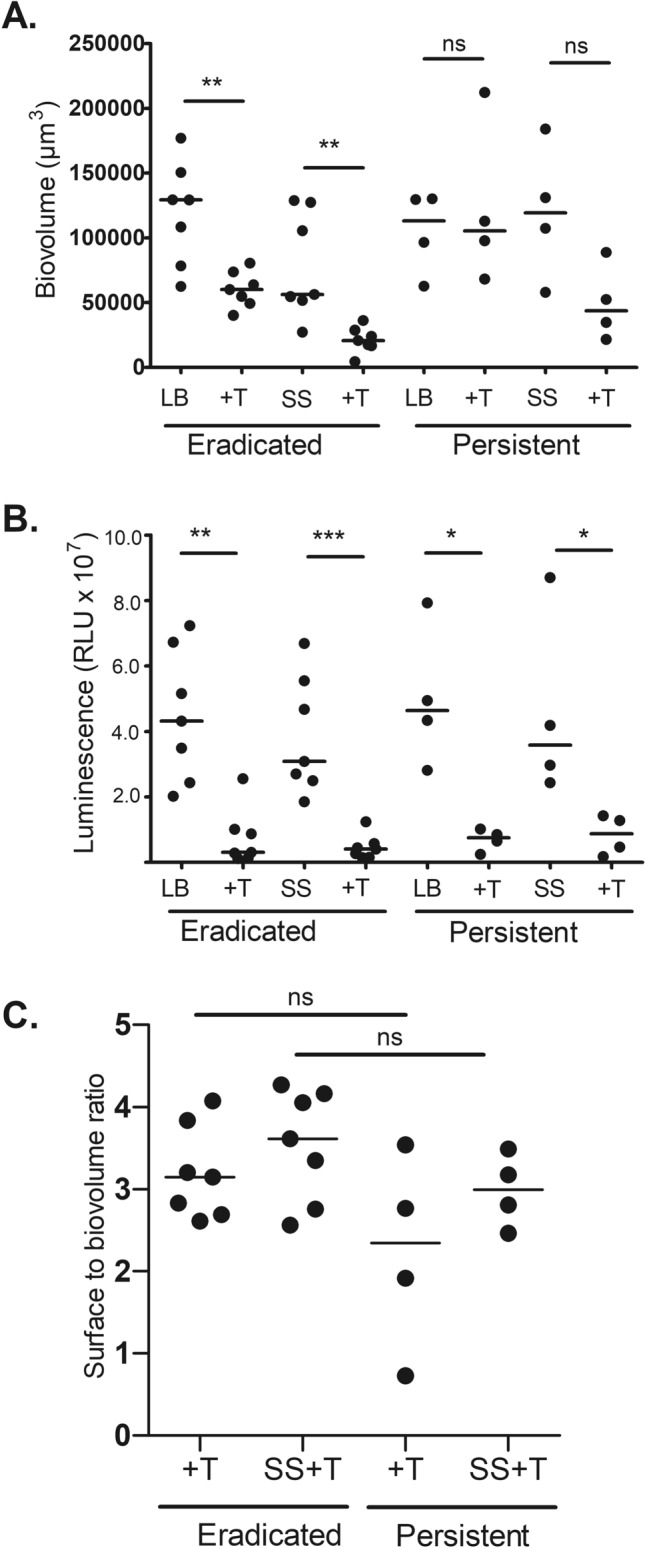
We previously demonstrated that P. aeruginosa isolates that persisted in children with cystic fibrosis (CF) despite inhaled tobramycin treatment had increased anti-Psl antibody binding in vitro compared to those successfully eradicated. We aimed to validate these findings by directly visualizing P. aeruginosa in CF sputum. This was a prospective observational study of children with CF with new-onset P. aeruginosa infection who underwent inhaled tobramycin eradication treatment. Using microbial identification passive clarity technique (MiPACT), P. aeruginosa was visualized in sputum samples obtained before treatment and classified as persistent or eradicated based on outcomes. Pre-treatment isolates were also grown as biofilms in vitro. Of 11 patients enrolled, 4 developed persistent infection and 7 eradicated infection. P. aeruginosa biovolume and the number as well as size of P. aeruginosa aggregates were greater in the sputum of those with persistent compared with eradicated infections (p < 0.01). The amount of Psl antibody binding in sputum was also greater overall (p < 0.05) in samples with increased P. aeruginosa biovolume. When visualized in sputum, P. aeruginosa had a greater biovolume, with more expressed Psl, and formed more numerous, larger aggregates in CF children who failed eradication therapy compared to those who successfully cleared their infection.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Gascon Casaredi, I. S. M., Waters, V., Seeto, R., Blanchard, A., Ratjen, F. Impact of antibiotic eradication therapy of Pseudomonas aeruginosa on long term lung function in cystic fibrosis. J. Cystic Fibros. (2022) (in press). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
