

Effects of Mindfulness Training and Exercise on Cognitive Function in Older Adults: A Randomized Clinical Trial
- PMID: 36511926
- PMCID: PMC9856438
- DOI: 10.1001/jama.2022.21680
Effects of Mindfulness Training and Exercise on Cognitive Function in Older Adults: A Randomized Clinical Trial
Abstract
Importance: Episodic memory and executive function are essential aspects of cognitive functioning that decline with aging. This decline may be ameliorable with lifestyle interventions.
Objective: To determine whether mindfulness-based stress reduction (MBSR), exercise, or a combination of both improve cognitive function in older adults.
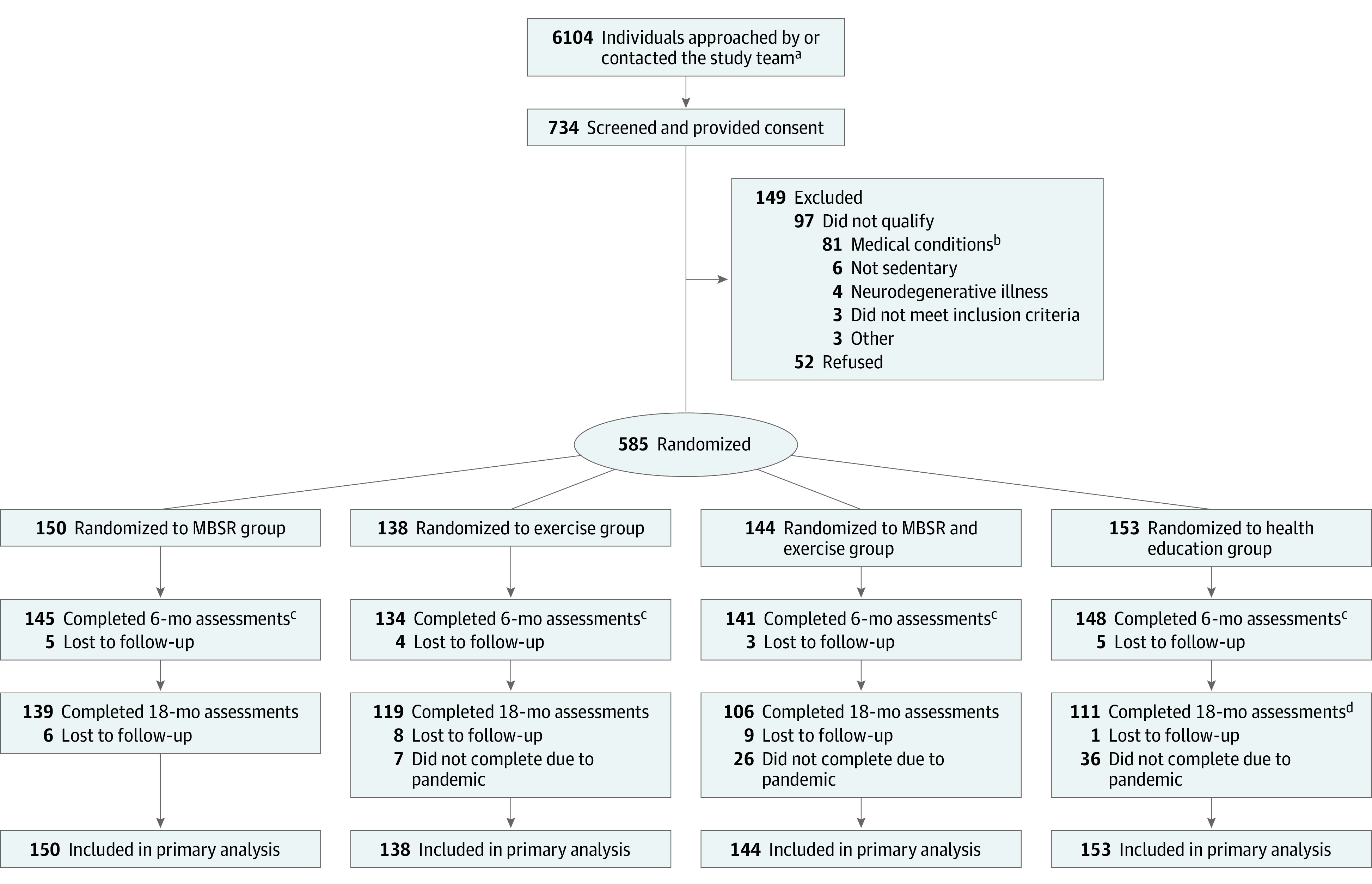
Design, setting, and participants: This 2 × 2 factorial randomized clinical trial was conducted at 2 US sites (Washington University in St Louis and University of California, San Diego). A total of 585 older adults (aged 65-84 y) with subjective cognitive concerns, but not dementia, were randomized (enrollment from November 19, 2015, to January 23, 2019; final follow-up on March 16, 2020).
Interventions: Participants were randomized to undergo the following interventions: MBSR with a target of 60 minutes daily of meditation (n = 150); exercise with aerobic, strength, and functional components with a target of at least 300 minutes weekly (n = 138); combined MBSR and exercise (n = 144); or a health education control group (n = 153). Interventions lasted 18 months and consisted of group-based classes and home practice.
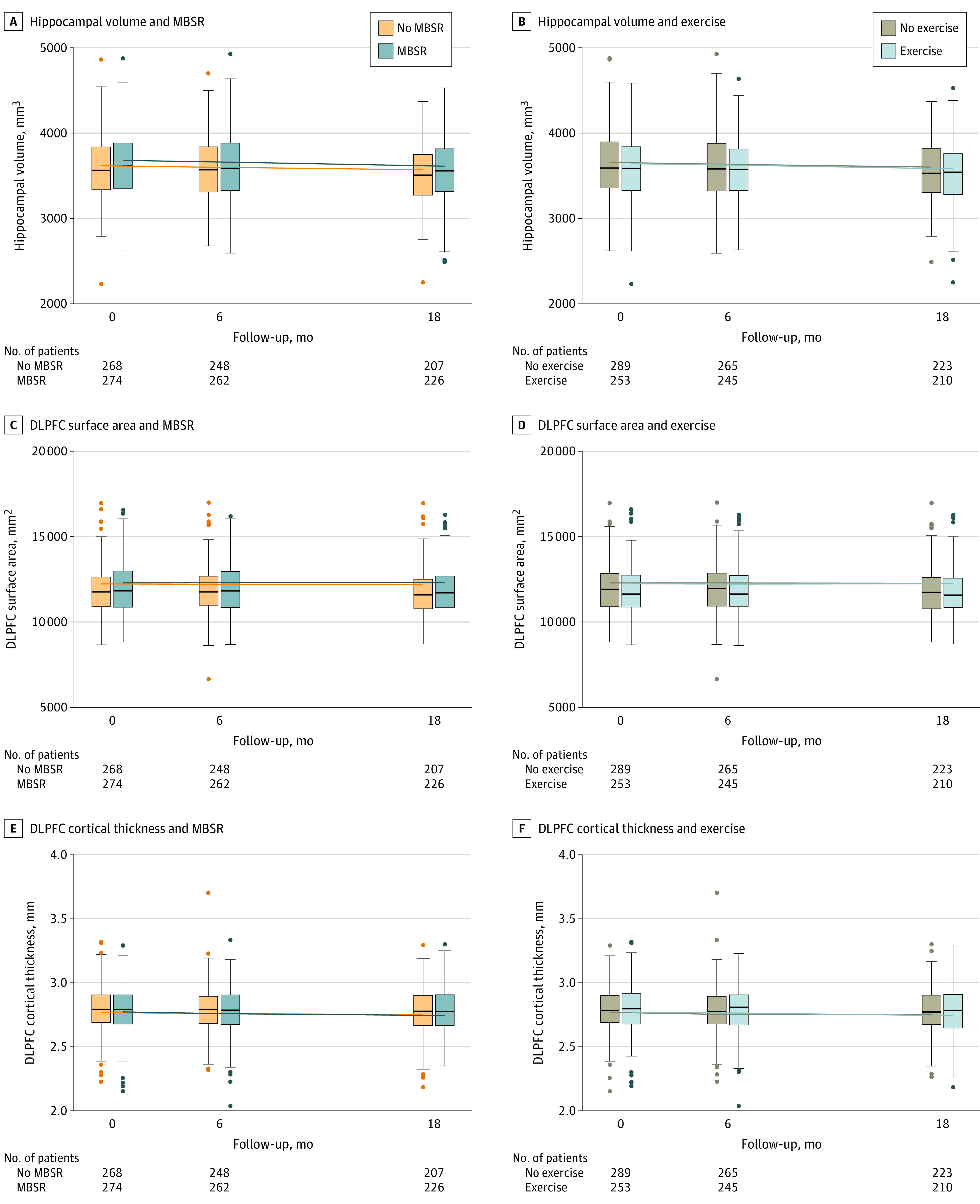
Main outcomes and measures: The 2 primary outcomes were composites of episodic memory and executive function (standardized to a mean [SD] of 0 [1]; higher composite scores indicate better cognitive performance) from neuropsychological testing; the primary end point was 6 months and the secondary end point was 18 months. There were 5 reported secondary outcomes: hippocampal volume and dorsolateral prefrontal cortex thickness and surface area from structural magnetic resonance imaging and functional cognitive capacity and self-reported cognitive concerns.
Results: Among 585 randomized participants (mean age, 71.5 years; 424 [72.5%] women), 568 (97.1%) completed 6 months in the trial and 475 (81.2%) completed 18 months. At 6 months, there was no significant effect of mindfulness training or exercise on episodic memory (MBSR vs no MBSR: 0.44 vs 0.48; mean difference, -0.04 points [95% CI, -0.15 to 0.07]; P = .50; exercise vs no exercise: 0.49 vs 0.42; difference, 0.07 [95% CI, -0.04 to 0.17]; P = .23) or executive function (MBSR vs no MBSR: 0.39 vs 0.31; mean difference, 0.08 points [95% CI, -0.02 to 0.19]; P = .12; exercise vs no exercise: 0.39 vs 0.32; difference, 0.07 [95% CI, -0.03 to 0.18]; P = .17) and there were no intervention effects at the secondary end point of 18 months. There was no significant interaction between mindfulness training and exercise (P = .93 for memory and P = .29 for executive function) at 6 months. Of the 5 prespecified secondary outcomes, none showed a significant improvement with either intervention compared with those not receiving the intervention.
Conclusions and relevance: Among older adults with subjective cognitive concerns, mindfulness training, exercise, or both did not result in significant differences in improvement in episodic memory or executive function at 6 months. The findings do not support the use of these interventions for improving cognition in older adults with subjective cognitive concerns.
Trial registration: ClinicalTrials.gov Identifier: NCT02665481.
Conflict of interest statement
Figures

Comment in
-
Mindfulness Training and Exercise and Cognitive Function in Older Adults.JAMA. 2023 Apr 4;329(13):1119-1120. doi: 10.1001/jama.2023.1448. JAMA. 2023. PMID: 37014344 No abstract available.
Similar articles
-
Mindfulness-based stress reduction for older adults with worry symptoms and co-occurring cognitive dysfunction.Int J Geriatr Psychiatry. 2014 Oct;29(10):991-1000. doi: 10.1002/gps.4086. Epub 2014 Feb 18. Int J Geriatr Psychiatry. 2014. PMID: 24677282 Free PMC article.
-
Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain: A Randomized Clinical Trial.JAMA. 2016 Mar 22-29;315(12):1240-9. doi: 10.1001/jama.2016.2323. JAMA. 2016. PMID: 27002445 Free PMC article. Clinical Trial.
-
Effects of home-based exercise alone or combined with cognitive training on cognition in community-dwelling older adults: A randomized clinical trial.Exp Gerontol. 2024 Dec;198:112628. doi: 10.1016/j.exger.2024.112628. Epub 2024 Nov 9. Exp Gerontol. 2024. PMID: 39505286 Clinical Trial.
-
Mindfulness-Based Stress Reduction and Mindfulness-Based Cognitive Therapy with Older Adults: A Qualitative Review of Randomized Controlled Outcome Research.Clin Gerontol. 2019 Jul-Sep;42(4):347-358. doi: 10.1080/07317115.2018.1518282. Epub 2018 Sep 11. Clin Gerontol. 2019. PMID: 30204557 Review.
-
Mindfulness and bodily distress.Dan Med J. 2012 Nov;59(11):B4547. Dan Med J. 2012. PMID: 23171754 Review.
Cited by
-
Effects of Mindfulness-Based Interventions (MBIs) in Patients with Early-Stage Alzheimer's Disease: A Pilot Study.Brain Sci. 2023 Mar 13;13(3):484. doi: 10.3390/brainsci13030484. Brain Sci. 2023. PMID: 36979294 Free PMC article.
-
From Breath to Strength: Does Mindfulness Improve Handgrip Strength Among Older Adults in India? A Propensity Score Matching Analysis.Psychogeriatrics. 2025 Jul;25(4):e70057. doi: 10.1111/psyg.70057. Psychogeriatrics. 2025. PMID: 40545251 Free PMC article.
-
Systematic review and meta-analysis of randomized controlled trials on the effects of exercise interventions on amyloid beta levels in humans.Exp Brain Res. 2024 May;242(5):1011-1024. doi: 10.1007/s00221-024-06821-y. Epub 2024 Mar 29. Exp Brain Res. 2024. PMID: 38551691
-
Data-driven clustering approach to identify novel clusters of high cognitive impairment risk among Chinese community-dwelling elderly people with normal cognition: A national cohort study.J Glob Health. 2024 Apr 19;14:04088. doi: 10.7189/jogh.14.04088. J Glob Health. 2024. PMID: 38638099 Free PMC article.
-
Cognitive, psychological, and physiological effects of a web-based mindfulness intervention in older adults during the COVID-19 pandemic: an open study.BMC Geriatr. 2024 Feb 14;24(1):151. doi: 10.1186/s12877-024-04766-z. BMC Geriatr. 2024. PMID: 38350854 Free PMC article.
