

A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Phase 2b Trial of P2X3 Receptor Antagonist Sivopixant for Refractory or Unexplained Chronic Cough
- PMID: 36512069
- PMCID: PMC9745691
- DOI: 10.1007/s00408-022-00592-5
A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Phase 2b Trial of P2X3 Receptor Antagonist Sivopixant for Refractory or Unexplained Chronic Cough
Abstract
Introduction: To determine the optimal dose of sivopixant, a highly selective P2X3 receptor antagonist, for refractory or unexplained chronic cough (RCC/UCC).
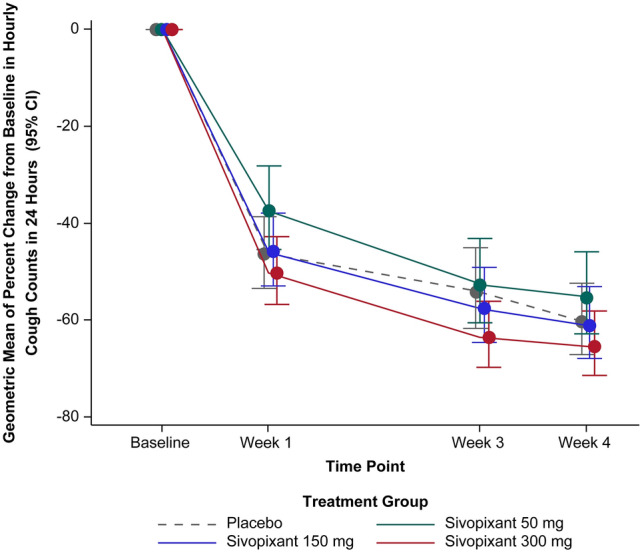
Methods: In this phase 2b, randomized, double-blind, placebo-controlled, parallel-group, multicenter trial, patients received sivopixant 50, 150, or 300 mg or placebo once daily for 4 weeks. The primary endpoint was a change from baseline in 24-h cough frequency (coughs/h) with sivopixant vs placebo.
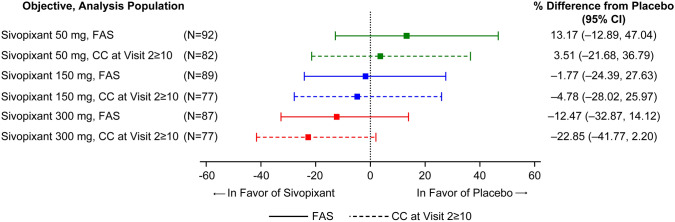
Results: Overall, 390/406 randomized patients completed the study. Placebo-adjusted changes in hourly cough count over 24 h were 13.17% (P = 0.3532), - 1.77% (P = 0.8935), and - 12.47% (P = 0.3241) and in cough severity (visual analog scale) were 1.75 mm (P = 0.5854), - 1.21 mm (P = 0.7056), and - 6.55 mm (P = 0.0433) with sivopixant 50, 150, and 300 mg, respectively. Placebo-adjusted changes from baseline in Leicester Cough Questionnaire total scores were - 0.37 (P = 0.4207), - 0.07 (P = 0.8806), and 0.69 (P = 0.1473) with sivopixant 50, 150, and 300 mg, respectively. Additionally, 61.3%, 78.3%, 86.8%, and 71.4% of patients receiving sivopixant 50, 150, and 300 mg and placebo, respectively, reported any improvements in Patient Global Impression of Change. The incidence of treatment-emergent adverse events (TEAEs) was 25.7%, 32.0%, 49.0%, and 20.6% in sivopixant 50, 150, and 300 mg and placebo groups, respectively; all TEAEs in the sivopixant group were mild-to-moderate.
Conclusion: Sivopixant did not demonstrate a statistically significant difference vs placebo in change from baseline in 24-h cough frequency. The dose of 300 mg has potential for RCC/UCC, showing the greatest improvements in cough frequency and patient-reported outcomes and dose-related mild to moderate reversible taste disturbance, although further trials are needed.
Clinical trial registration: ClinicalTrials.gov identifier NCT04110054; registered September 26, 2019.
Keywords: Chronic cough; Cough frequency; P2X3 receptor antagonist; Phase 2b trial; Sivopixant.
© 2022. The Author(s).
Conflict of interest statement
LMG has received grants or contracts and consulting fees from Shionogi Inc., Bayer, Merck, Bellus Health, and Chiesi; consulting fees from AstraZeneca, Nocion, Trevi Therapeutics, Reckitt Benckiser Health Limited, NeRRe Therapeutics, and Bionorica; payment or honoraria from Merck, Chiesi, Bellus, Bionorica, GSK, and Shionogi Inc. and participated on a Data Safety Monitoring Board or the Advisory Board for Applied Clinical Intelligence. JAS has served as a consultant and helped in the setup of clinical studies for Shionogi; received grants or contracts from Wellcome Trust investigator award and NIHR Manchester Biomedical Research Centre; her hospital has received royalties from Vitalograph Ltd.; received consulting fee from Bellus Health, Axalbion, Merck, Bayer, Algernon, Nocion, Chiesi, Boehringer Ingelheim, and AstraZeneca; received honoraria from Merck and Boehringer Ingelheim; has a patent issued for cough monitoring; and received equipment supply from Vitalograph Ltd. AMo has received funding from Shionogi; received payment or honoraria from Merck, Bayer, and NeRRe; participated on a Data Safety Monitoring Board or an Advisory Board for Merck, Bayer, NeRRe, Shionogi, and Bellus; and served as the task force chair for the European Respiratory Society. SSB has received personal fees from Shionogi Inc., Merck, Bellus, Bayer, and Nocion. KFC has speaking engagements for Novartis and AstraZeneca; has participated on Advisory Boards for Roche, Merck, Reckitt Benckiser, and Shionogi & Co., Ltd., on asthma, COPD, and chronic cough; serves on Data Safety Monitoring Board for Nocion; and has received grants including MRC grant on Precision Medicine for severe asthma, an EPSRC grant on air pollution and asthma, and a GSK grant on mepolizumab and eosinophils in asthma. PVD has served as a consultant to Bayer, Bellus, Chiesi, Merck, and Shionogi Inc. and is the editor-in-chief of
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
