

Ultrasound imaging of bone fractures
- PMID: 36512142
- PMCID: PMC9748005
- DOI: 10.1186/s13244-022-01335-z
Ultrasound imaging of bone fractures
Abstract
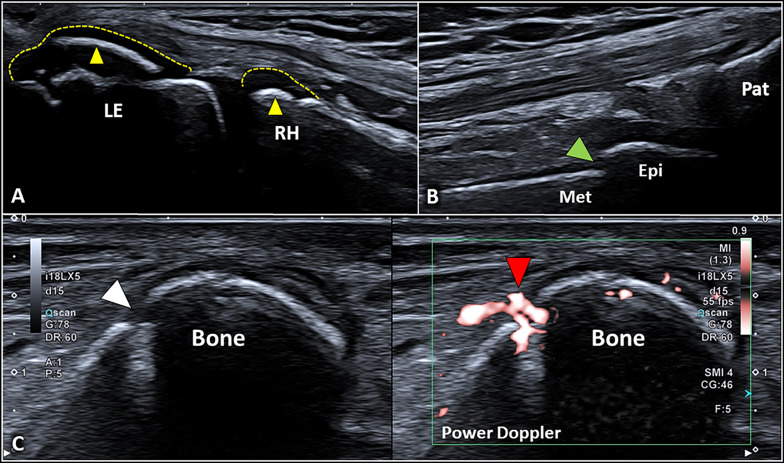
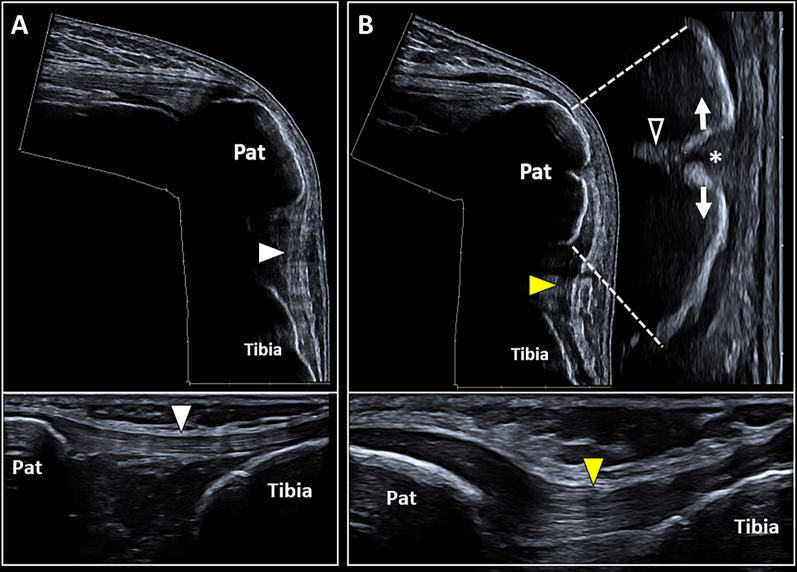
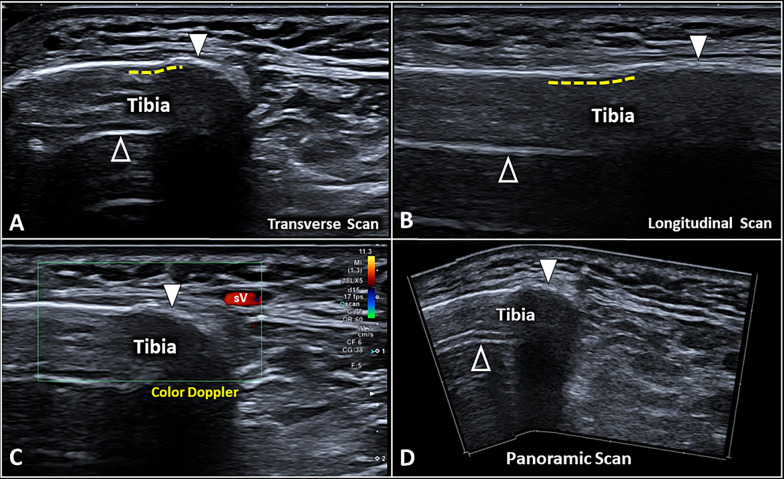
Ultrasound imaging is widely used to evaluate the neuromusculoskeletal system, and recently, a particular interest is mounting in assessing the bone tissue and fractures. Ultrasound can be considered a valuable diagnostic tool to perform a first-line evaluation of bone tissue, especially in particular settings without direct access to X-ray imaging and/or in emergency conditions. Moreover, different healing phases of bone fractures can be accurately assessed by combining the B-mode modality and (high-sensitive) color/power Doppler optimizing the management of patients-e.g., planning of progressive loads and rehabilitation procedures. In this review, we summarized the role of ultrasound imaging in the management of bone fractures and described the most common sonographic signs encountered in the daily practice by assessing different types of bone fractures and the progressive phases of the healing process.
Keywords: Bone fracture; Fracture healing; Ultrasound.
© 2022. The Author(s).
Conflict of interest statement
Andrea Delli Pizzi and Antonio Corvino are members of the Insights into Imaging Editorial Board. They have not taken part in the review or selection process of this article. All remaining authors state no conflict of interest.
Figures



References
-
- Wang CC, Linden KL, Otero HJ. Sonographic evaluation of fractures in children. J Diagn Med Sonogr. 2017;33(3):200–207. doi: 10.1177/8756479316688897. - DOI
Publication types
LinkOut - more resources
Full Text Sources
