

Hospitalizations Associated With Mental Health Conditions Among Adolescents in the US and France During the COVID-19 Pandemic
- PMID: 36512353
- PMCID: PMC9856226
- DOI: 10.1001/jamanetworkopen.2022.46548
Hospitalizations Associated With Mental Health Conditions Among Adolescents in the US and France During the COVID-19 Pandemic
Abstract
Importance: The COVID-19 pandemic has been associated with an increase in mental health diagnoses among adolescents, though the extent of the increase, particularly for severe cases requiring hospitalization, has not been well characterized. Large-scale federated informatics approaches provide the ability to efficiently and securely query health care data sets to assess and monitor hospitalization patterns for mental health conditions among adolescents.
Objective: To estimate changes in the proportion of hospitalizations associated with mental health conditions among adolescents following onset of the COVID-19 pandemic.
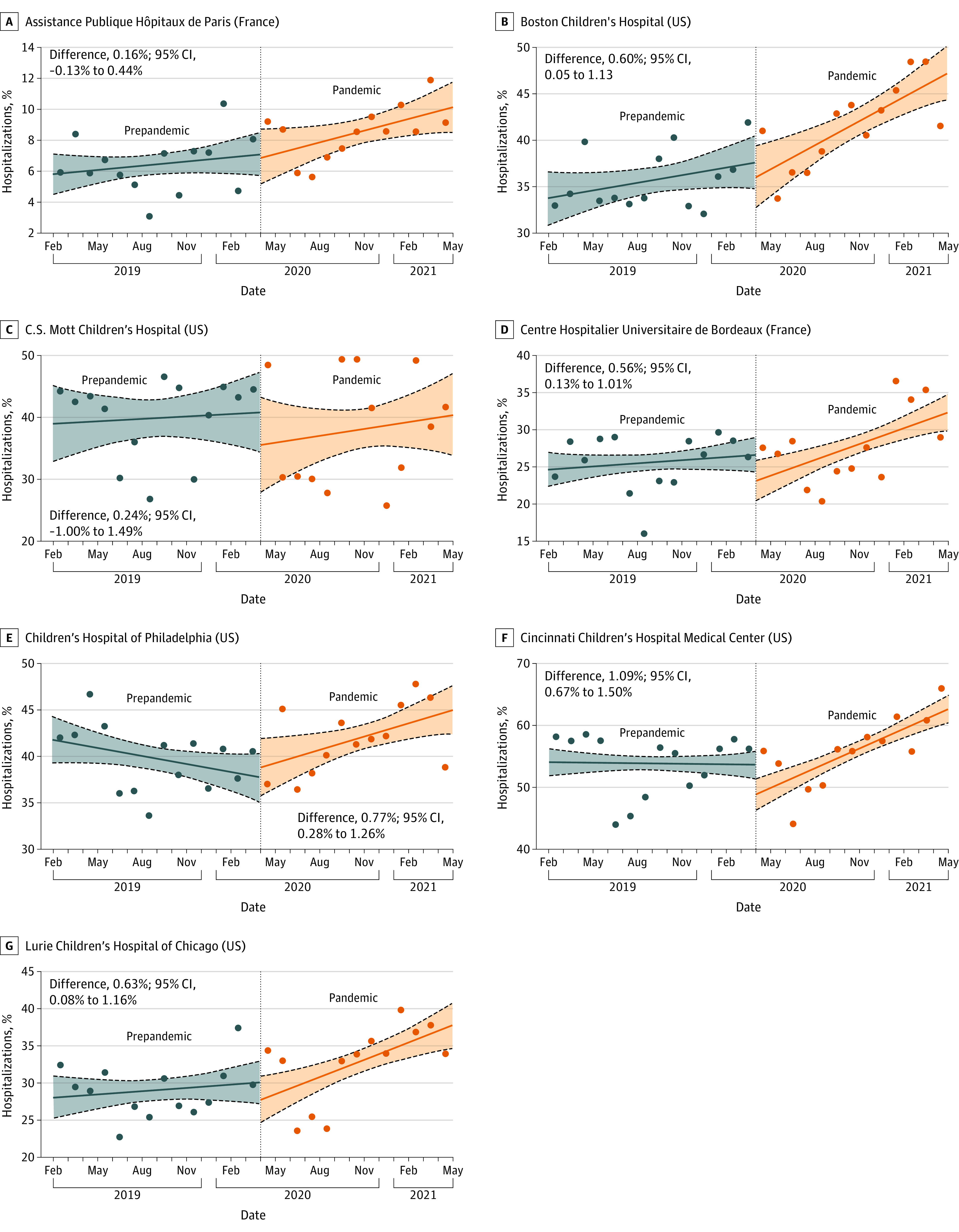
Design, setting, and participants: This retrospective, multisite cohort study of adolescents 11 to 17 years of age who were hospitalized with at least 1 mental health condition diagnosis between February 1, 2019, and April 30, 2021, used patient-level data from electronic health records of 8 children's hospitals in the US and France.
Main outcomes and measures: Change in the monthly proportion of mental health condition-associated hospitalizations between the prepandemic (February 1, 2019, to March 31, 2020) and pandemic (April 1, 2020, to April 30, 2021) periods using interrupted time series analysis.
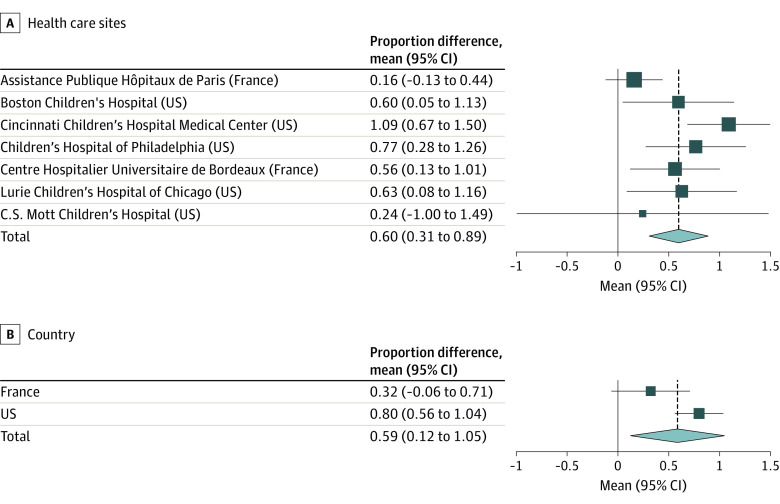
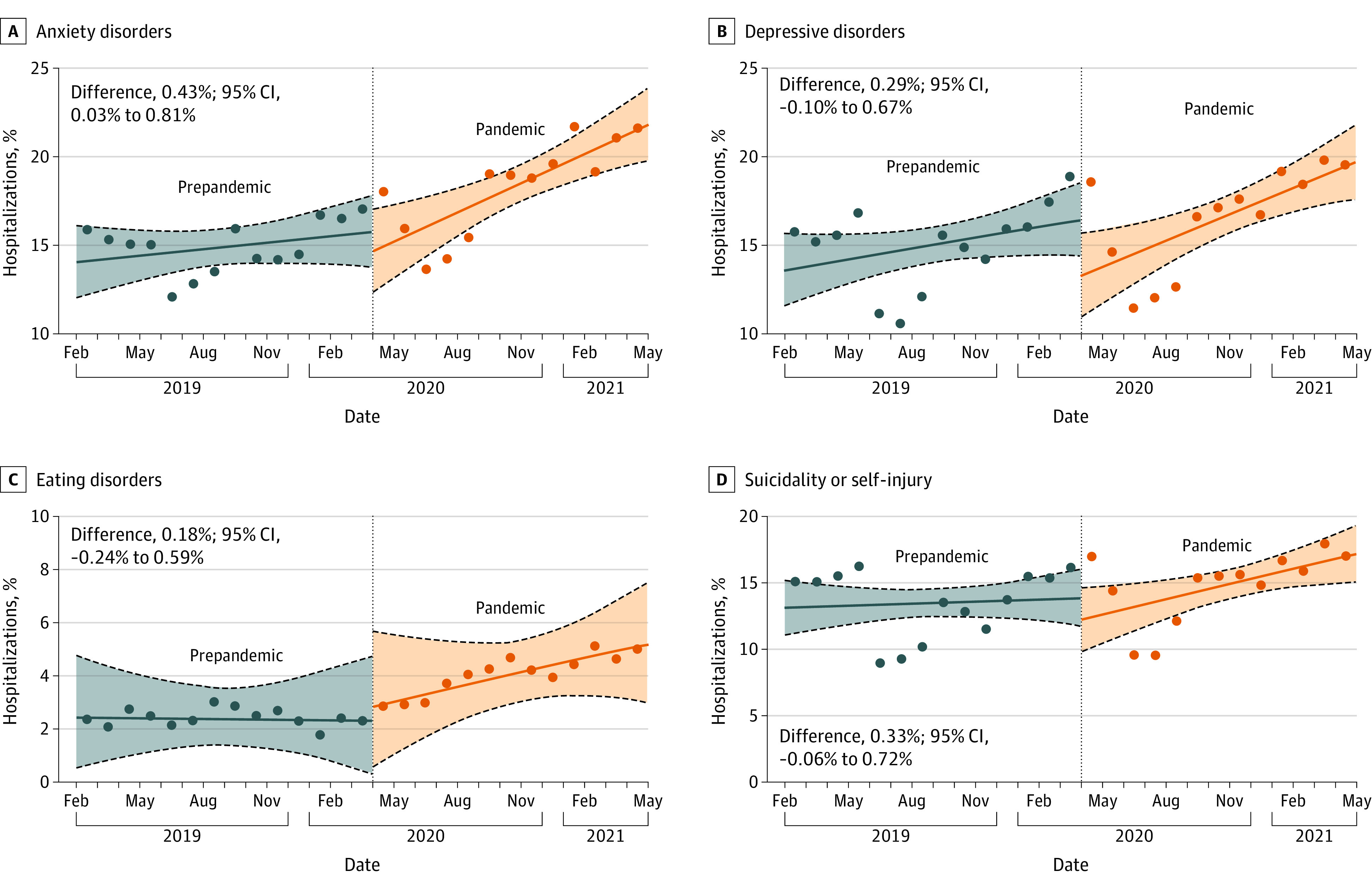
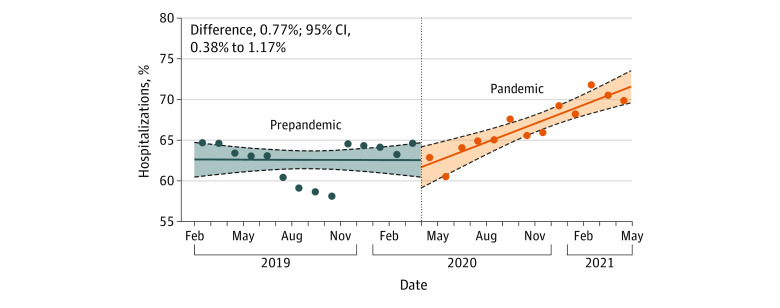
Results: There were 9696 adolescents hospitalized with a mental health condition during the prepandemic period (5966 [61.5%] female) and 11 101 during the pandemic period (7603 [68.5%] female). The mean (SD) age in the prepandemic cohort was 14.6 (1.9) years and in the pandemic cohort, 14.7 (1.8) years. The most prevalent diagnoses during the pandemic were anxiety (6066 [57.4%]), depression (5065 [48.0%]), and suicidality or self-injury (4673 [44.2%]). There was an increase in the proportions of monthly hospitalizations during the pandemic for anxiety (0.55%; 95% CI, 0.26%-0.84%), depression (0.50%; 95% CI, 0.19%-0.79%), and suicidality or self-injury (0.38%; 95% CI, 0.08%-0.68%). There was an estimated 0.60% increase (95% CI, 0.31%-0.89%) overall in the monthly proportion of mental health-associated hospitalizations following onset of the pandemic compared with the prepandemic period.
Conclusions and relevance: In this cohort study, onset of the COVID-19 pandemic was associated with increased hospitalizations with mental health diagnoses among adolescents. These findings support the need for greater resources within children's hospitals to care for adolescents with mental health conditions during the pandemic and beyond.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
- U01 TR003528/TR/NCATS NIH HHS/United States
- T32 LM012203/LM/NLM NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- R01 NS098023/NS/NINDS NIH HHS/United States
- FS/19/52/34563/BHF_/British Heart Foundation/United Kingdom
- R01 LM013337/LM/NLM NIH HHS/United States
- P30 ES017885/ES/NIEHS NIH HHS/United States
- K23 HL148394/HL/NHLBI NIH HHS/United States
- R01 HL089778/HL/NHLBI NIH HHS/United States
- R01 NS124882/NS/NINDS NIH HHS/United States
- U24 HL148865/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- R01 HD105939/HD/NICHD NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- L40 HL148910/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
