

Estimating Risk of Antidepressant Withdrawal from a Review of Published Data
- PMID: 36513909
- PMCID: PMC9911477
- DOI: 10.1007/s40263-022-00960-y
Estimating Risk of Antidepressant Withdrawal from a Review of Published Data
Abstract
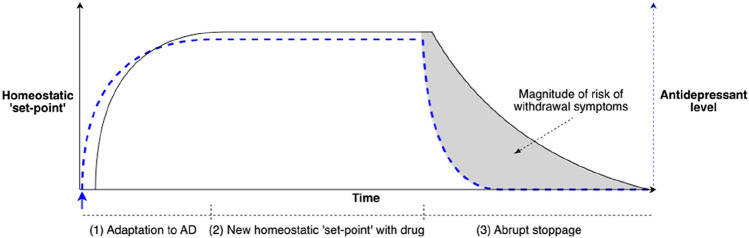
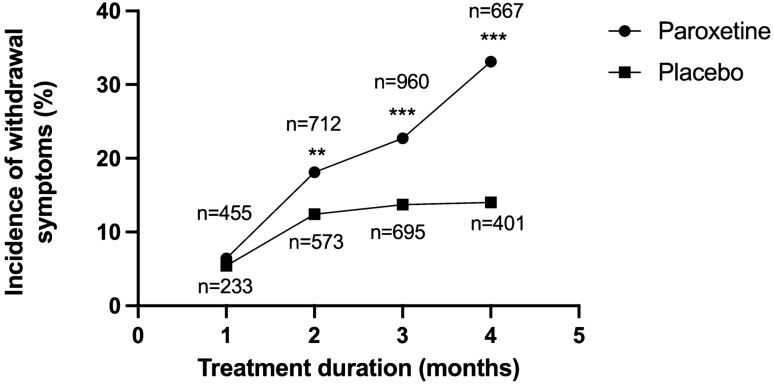
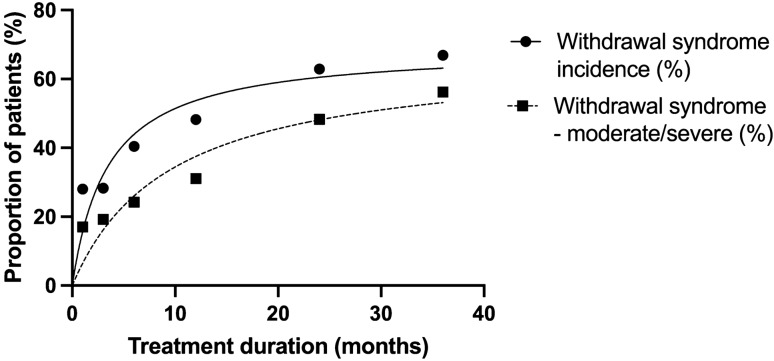
Adaptation of the brain to the presence of a drug predicts withdrawal on cessation. The outcome of adaptation is often referred to as 'physical dependence' in pharmacology, as distinct from addiction, although these terms have unfortunately become conflated in some diagnostic guides. Physical dependence to antidepressants may occur in some patients, consistent with the fact that some patients experience withdrawal effects from these medications. It is thought that longer duration of use, higher dose and specific antidepressants affect the risk of antidepressant withdrawal effects as they might cause greater adaptation of the brain. We searched PubMed for relevant systematic reviews and other relevant analyses to summarise existing data on determinants of antidepressant withdrawal incidence, severity and duration. Overall, data were limited. From survey data, increased duration of use was associated with an increased incidence and severity of withdrawal effects, consistent with some evidence from data provided by drug manufacturers. Duration of use may be related to duration of withdrawal effects but data are heterogenous and sparse. Serotonin and noradrenaline reuptake inhibitors and paroxetine are associated with higher risks than other antidepressants, though data for some antidepressants are lacking. Higher doses of antidepressant has some weak association with an increased risk of withdrawal, with some ceiling effects, perhaps reflecting receptor occupancy relationships. Past experience of withdrawal effects is known to predict future risk. Based on these data, we outline a preliminary rubric for determining the risk of withdrawal symptoms for a particular patient, which may have relevance for determining tapering rates. Given the limited scope of the current research, future research should aim to clarify prediction of antidepressant withdrawal risk, especially by examining the risk of withdrawal in long-term users of medication, as well as the severity and duration of effects, to improve the preliminary tool for predictive purposes. Further research into the precise adaptations in long-term antidepressant use may improve the ability to predict withdrawal effects for a particular patient.
© 2022. The Author(s).
Conflict of interest statement
Anders Sørensen has no conflicts of interest. Mark Abie Horowitz declares that he is a co-founder of Outro Health, a company aiming to help people safely stop unnecessary antidepressants in Canada and North America. Adele Framer declares she is a co-founder of Outro Health. Michael P. Hengartner reports royalties from Palgrave Macmillan, London, UK for his book published in December, 2021, called “Evidence-biased Antidepressant Prescription.” David Taylor reports grants and personal fees from Janssen, Sunovion, Recordati and Mylan, and personal fees from Accord, outside the submitted work.
Figures
References
-
- NHS Business Services Authority. Medicines used in mental health England 2015/16 to 2019/20. 2020. Available from: https://nhsbsa-opendata.s3-eu-west-2.amazonaws.com/mh-annual-narrative-f.... Accessed 4 May 2021.
-
- Public Health England. Dependence and withdrawal associated with some prescribed medicines: an evidence review. 2019. Available from: https://www.gov.uk/government/publications/prescribed-medicines-review-r.... Accessed 25 May 2021.
-
- Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: are guidelines evidence-based? Addict Behav. 2019;97:111–121. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
