

Associations of Metabolic Syndrome and Abdominal Obesity with Anion Gap Metabolic Acidosis among US Adults
- PMID: 36514392
- PMCID: PMC9717647
- DOI: 10.34067/KID.0002402022
Associations of Metabolic Syndrome and Abdominal Obesity with Anion Gap Metabolic Acidosis among US Adults
Abstract
Background: Obesity is a recently identified risk factor for metabolic acidosis and anion gap elevations in the absence of CKD. Metabolic acidosis is a treatable condition with substantial adverse effects on human health. Additional investigations are needed to characterize at-risk populations and explore potential mechanisms. We hypothesized metabolic syndrome (MetS) and waist circumference (WC) would be closely associated with this pathology.
Methods: Adult participants from NHANES 1999-2018 meeting study criteria were compiled as main (n=31,163) and fasting (n=12,860) cohorts. Regression models adjusted for dietary acid, eGFR, and other factors examined associations of WC and MetS features with anion gap metabolic acidosis and its components (serum bicarbonate ≤23 mEq/L and anion gap >95th percentile).
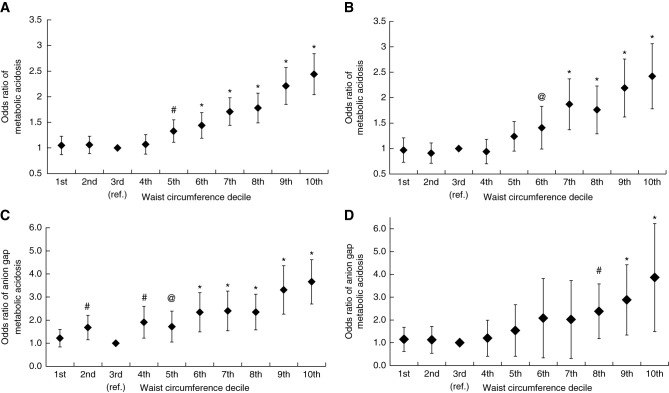
Results: Greater WC and MetS features were associated with progressively lower bicarbonate, higher anion gap, and greater odds ratios (OR) of metabolic acidosis (MA) and anion gap metabolic acidosis (AGMA). Compared with the reference, participants with the highest WC had ORs for MA and AGMA of 2.26; 95% CI, 1.96 to 2.62 and 2.89; 95% CI, 1.97 to 4.21; those with three and four versus zero MetS features had ORs for AGMA of 2.52; 95% CI, 1.95 to 2.94 and 3.05; 95% CI, 2.16 to 3.82. Associations of body mass index with outcomes were attenuated or absent after adjustment for WC or MetS. Findings were preserved after excluding eGFR <90 ml/min per 1.73 m2 and albuminuria. A lower MA cutoff (<22 mEq/L) raised the estimate of association between MetS and MA (OR for three and four vs zero features: 3.56; 95% CI, 2.53 to 5.02 and 5.44; 95% CI, 3.66 to 8.08).
Conclusions: Metabolic diseases are characterized by metabolic acidosis and anion gap elevations. Metabolic dysfunction may predispose patients without CKD to systemic acidosis from endogenous sources. Comprehensive acid-base analyses may be informative in patients with metabolic diseases.
Keywords: abdominal obesity; acid-base equilibrium; acid/base and electrolyte disorders; anion gap; metabolic acidosis; metabolic syndrome; obesity; waist circumference.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
J. Kane reports having an advisory or leadership role with the Eli Lilly obesity advisory board (will be serving from August 2022). M.K. Abramowitz reports having consultancy agreements with Tricida; and reports having an ownership interest in Aethlon Medical, Inc. All remaining authors have nothing to disclose.
Figures


Comment in
-
Minding the Gap Beyond Kidney Disease: Utility of the Anion Gap in Metabolic Syndrome.Kidney360. 2022 Nov 24;3(11):1819-1822. doi: 10.34067/KID.0005142022. eCollection 2022 Nov 24. Kidney360. 2022. PMID: 36514414 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
