

Right middle lobe syndrome after upper lobectomy: Role of the bronchial angle
- PMID: 36514840
- PMCID: PMC11199077
- DOI: 10.1177/02184923221144402
Right middle lobe syndrome after upper lobectomy: Role of the bronchial angle
Abstract
Background: Right middle lobe syndrome is part of a spectrum of relatively rare but serious conditions that may occur following right upper lobectomy. We aimed to assess whether the preoperative middle lobe bronchial angle on CT predicted patients at risk of developing middle lobe syndrome.
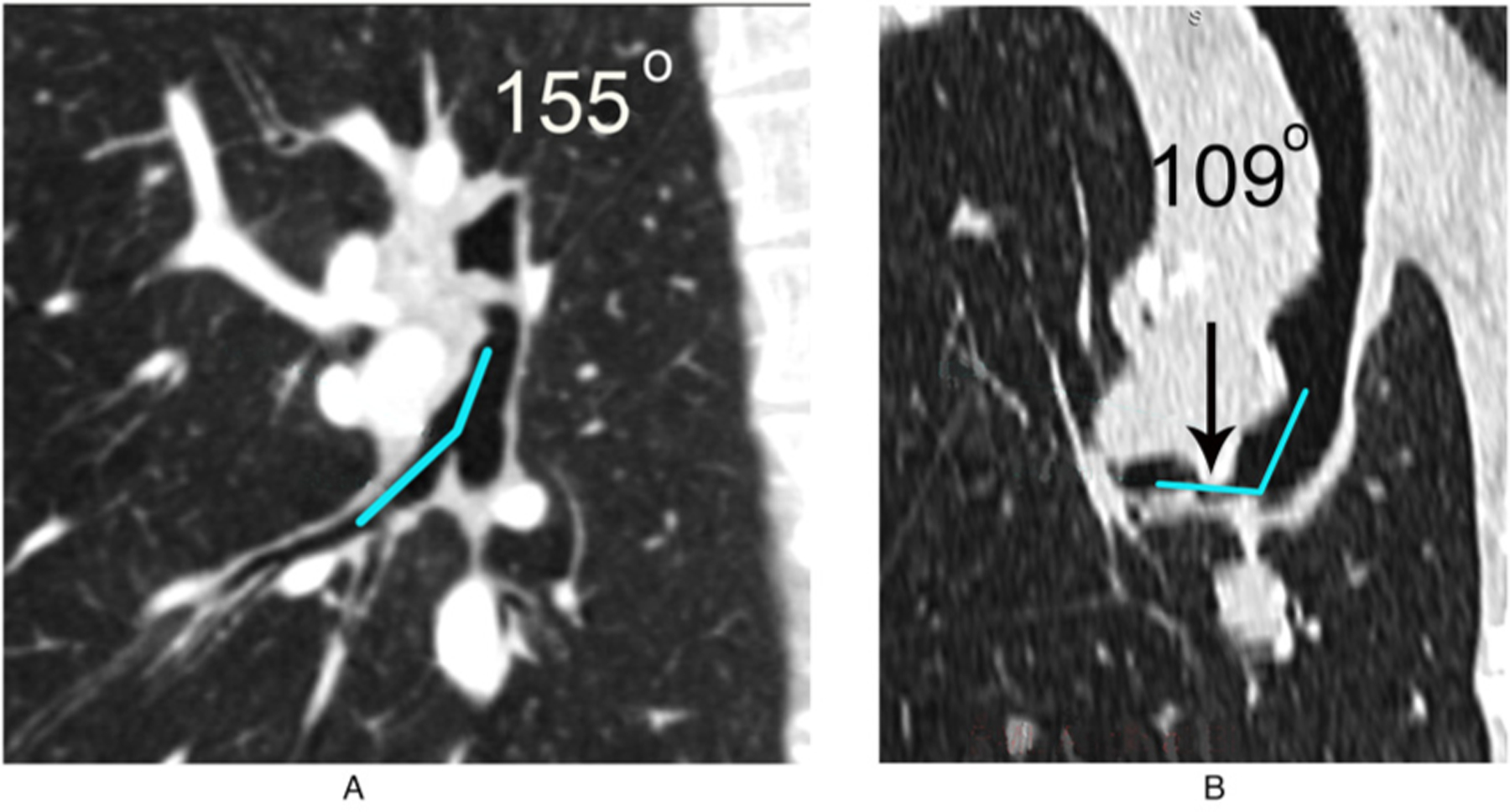
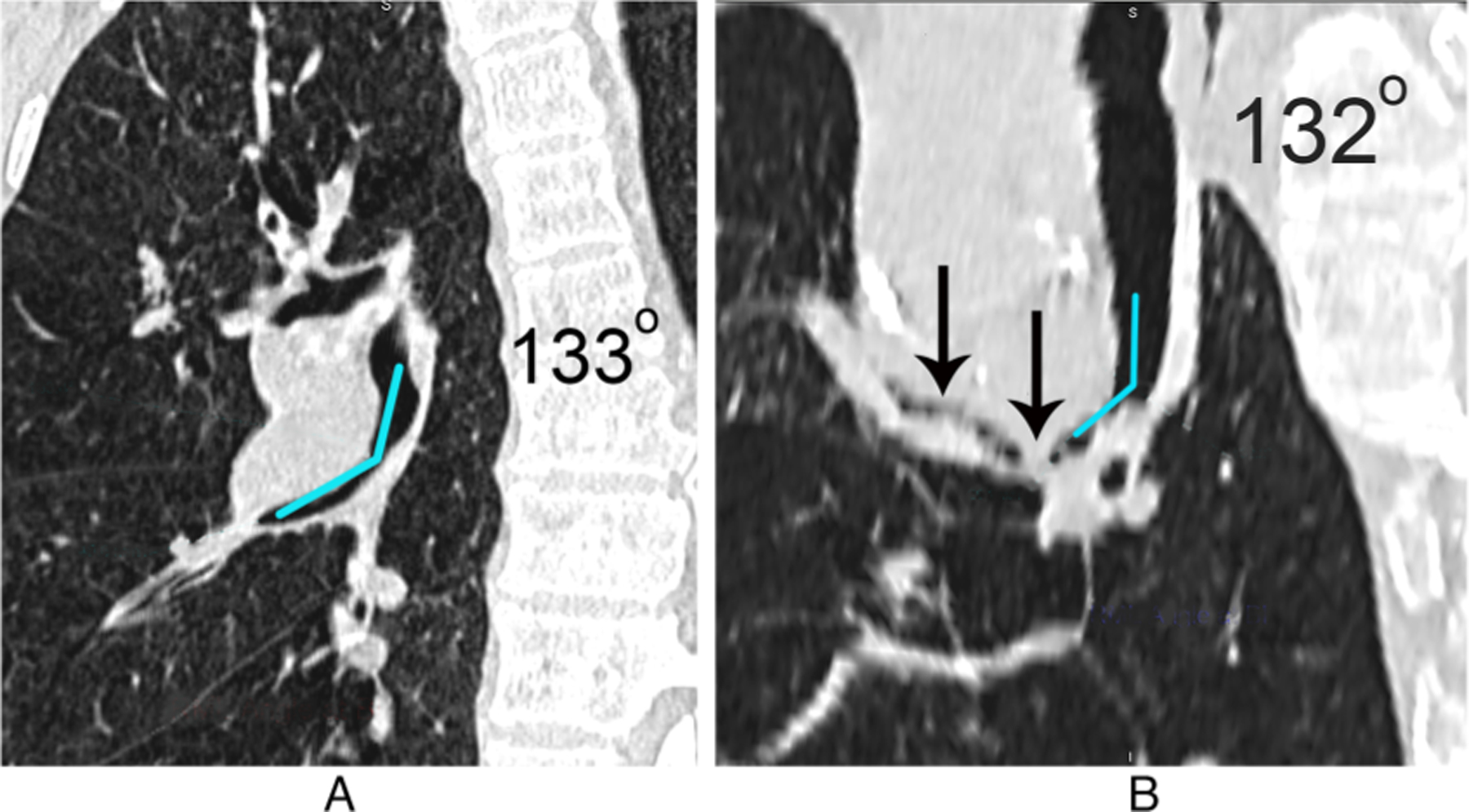
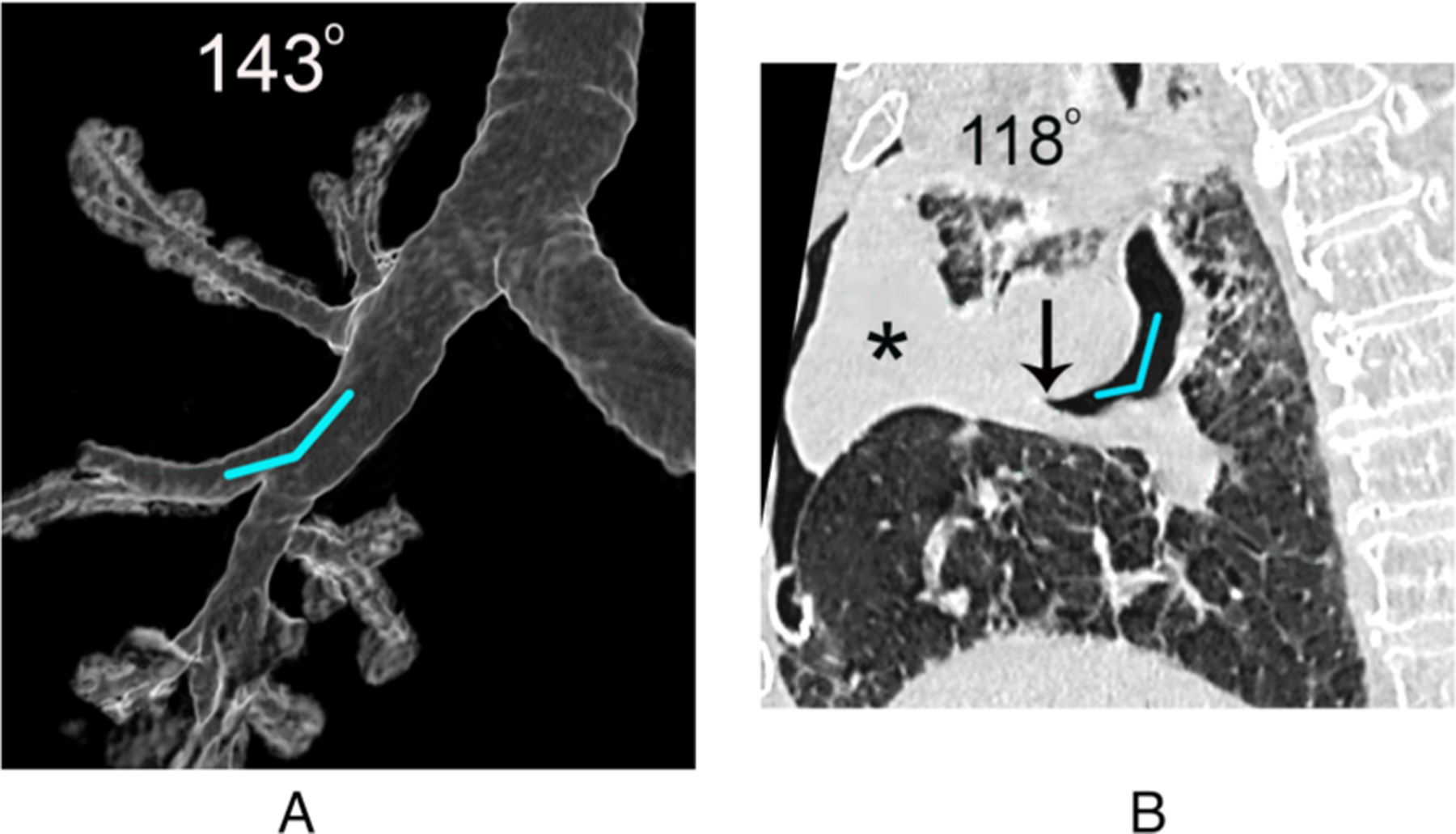
Method: All patients who had a complete upper lobectomy over 4 years were retrospectively reviewed for clinical and imaging findings of middle lobe syndrome. Patients with previous lung surgery, preoperative chemo- or radiation therapy, or more extensive surgical resection were excluded. Patient demographics and symptoms, the surgical, pathologic and bronchoscopy reports, and pre- and post-operative chest imaging, to include 3D CT reconstructions and measurements of the middle lobe angles in a subset of patients, were retrospectively reviewed.
Result: One hundred and twenty-eight patients met inclusion criteria. Ten (8%) had middle lobe syndrome based on symptoms and imaging features. Eight had severe middle lobe consolidation. Two had postoperative onset of wheezing, with middle lobe bronchial abnormality on CT. The pre- and postoperative middle lobe bronchial angles of 14 patients without middle lobe syndrome were compared to 10 patients with middle lobe syndrome. The middle lobe bronchus was completely obliterated postoperatively and could not be determined in 1 patient. There was no significant difference between the pre- and postoperative angles in patients with or without middle lobe syndrome.
Conclusion: Middle lobe syndrome occurred in 8% of patients with right upper lobectomy. The preoperative middle lobe bronchial angle did not predict patients at risk for developing middle lobe syndrome.
Conflict of interest statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Dai J, Xie D, Wang H, et al. Predictors of survival in lung torsion: a systematic review and pooled analysis. J Thorac Cardiovasc Surg 2016; 152: 737–745. - PubMed
-
- Liu SH, Wan FY and Chiang JB. Post-lobectomy lung torsion: report of two cases. Hong Kong J Radiol 2021; 24: 52–55.
-
- Kanaan S, Boswell WD and Hagen JA. Clinical and radiographic signs lead to early detection of lobar torsion and subsequent successful intervention. J Thorac Cardiovasc Surg 2006; 132: 720–721. - PubMed
-
- Sung HK, Kim HK and Choi YH. Re-thoracoscopic surgery for middle lobe torsion after right upper lobectomy. Eur J Cardiothorac Surg 2012; 42: 582–583. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
