

Change in Depressive Symptoms During the First Month of Discharge and 1-Year Clinical Outcomes in Patients Hospitalized for Heart Failure
- PMID: 36515248
- PMCID: PMC9798811
- DOI: 10.1161/JAHA.122.027438
Change in Depressive Symptoms During the First Month of Discharge and 1-Year Clinical Outcomes in Patients Hospitalized for Heart Failure
Abstract
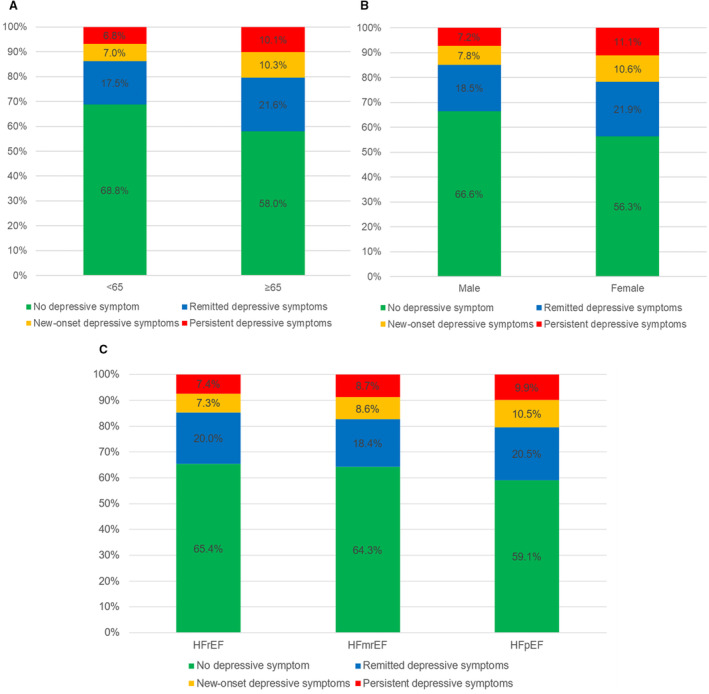
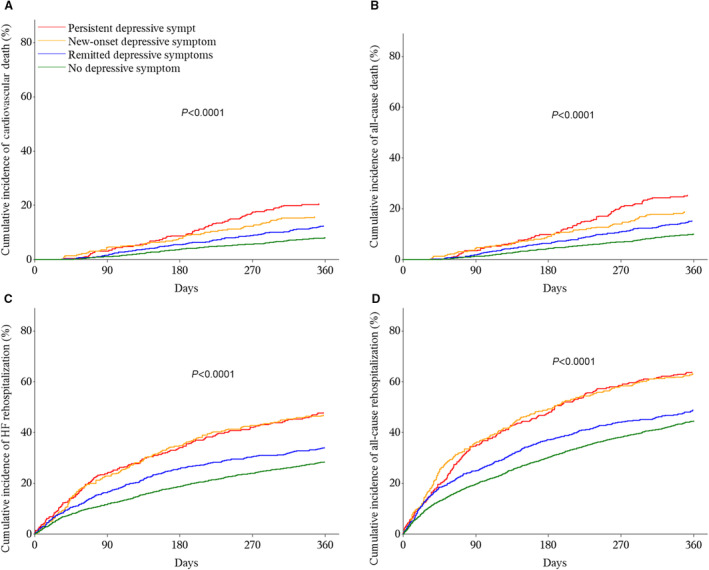
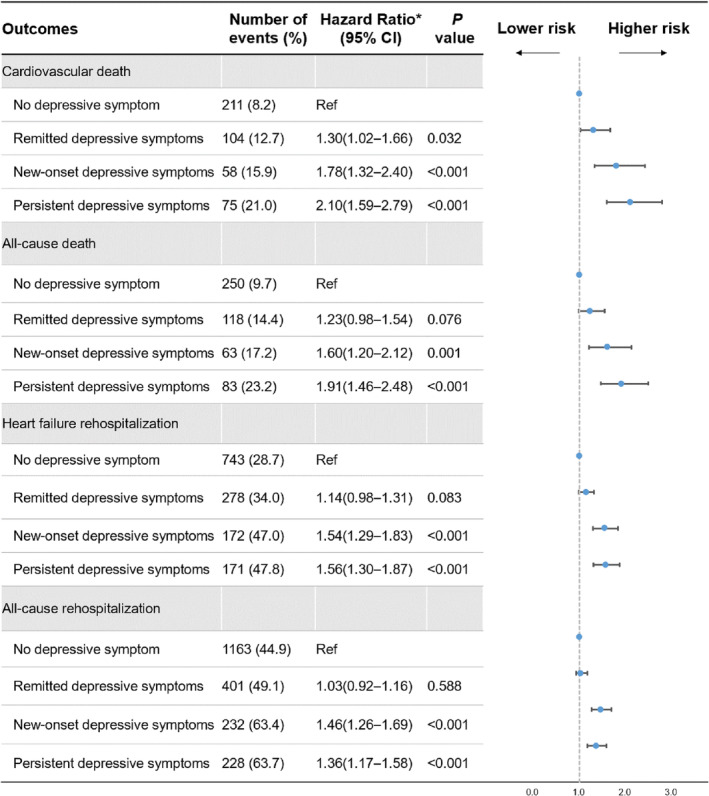
Background The patterns of depressive symptom change during the first month after discharge, as well as their prognostic implications, and predictors of persistent or new-onset depressive symptoms are not well characterized. Methods and Results We included patients hospitalized for heart failure undergoing Patient Health Questionnaire-2 before discharge and at 1 month after discharge in a multicenter prospective cohort. We characterized 4 patterns of change in depressive symptoms-persistent, new-onset, remitted depressive symptoms, and no depressive symptom-and examined the associations between the 4 patterns and 1-year clinical outcomes. We analyzed the factors associated with persistent or new-onset depressive symptoms. A total of 4130 patients were included. Among 1175 (28.5%) symptomatic patients and 2955 (71.5%) symptom-free patients before discharge, 817 (69.5%) had remission, and 366 (12.2%) had new-onset depressive symptoms, respectively. Compared with no depressive symptom, persistent depressive symptoms were associated with an increased risk of cardiovascular death (hazard ratio [HR], 2.10 [95% CI, 1.59-2.79]) and heart failure rehospitalization (HR, 1.56 [95% CI, 1.30-1.87]); new-onset depressive symptoms were associated with an increased risk of cardiovascular death (HR, 1.78 [95%CI, 1.32-2.40]) and heart failure rehospitalization (HR, 1.54 [95% CI, 1.29-1.83]). Remitted depressive symptoms were associated with a slightly increased risk of cardiovascular death but had no significant association with heart failure rehospitalization. Patients who were female or had poor socioeconomic status, stroke history, renal dysfunction, or poor health status had a higher risk of persistent or new-onset depressive symptoms. Conclusions Sex, socioeconomic status, clinical characteristics, and health status help identify patients with high risks of depressive symptoms at 1 month after discharge. Dynamic capture of depressive symptom change during this period informs long-term risk stratifications and targets patients who require psychological interventions and social support to improve clinical outcomes. Registration URL: https://www.clinicaltrials.gov; Unique identifier (NCT02878811).
Keywords: death; depressive symptom; heart failure; postdischarge period; rehospitalization.
Figures
Similar articles
-
Individual Trajectories of Health Status During the First Year of Discharge From Hospitalization for Heart Failure and Their Associations With Death in the Following Years.J Am Heart Assoc. 2023 Jul 18;12(14):e028782. doi: 10.1161/JAHA.122.028782. Epub 2023 Jul 8. J Am Heart Assoc. 2023. PMID: 37421271 Free PMC article. Clinical Trial.
-
Associations of cumulative depressive symptoms within 1-year of discharge with subsequent mortality among patients hospitalized for acute heart failure: Findings from The China PEACE Prospective Heart Failure Study.J Affect Disord. 2024 Apr 15;351:299-308. doi: 10.1016/j.jad.2024.01.245. Epub 2024 Jan 28. J Affect Disord. 2024. PMID: 38290578
-
Distinct Associations Between Postdischarge Cognitive Change Patterns and 1-year Outcomes in Patients Hospitalized for Heart Failure.J Card Fail. 2023 Jun;29(6):870-879. doi: 10.1016/j.cardfail.2023.01.006. Epub 2023 Feb 9. J Card Fail. 2023. PMID: 36764442
-
Risk Factors and Clinical Outcomes of Nonhome Discharge in Patients With Acute Decompensated Heart Failure: An Observational Study.J Am Heart Assoc. 2021 Aug 3;10(15):e020292. doi: 10.1161/JAHA.120.020292. Epub 2021 Jul 30. J Am Heart Assoc. 2021. PMID: 34325523 Free PMC article.
-
Comparative potential of the 2-item versus the 9-item patient health questionnaire to predict death or rehospitalization in heart failure.Circ Heart Fail. 2015 May;8(3):464-72. doi: 10.1161/CIRCHEARTFAILURE.114.001488. Epub 2015 Apr 15. Circ Heart Fail. 2015. PMID: 25878325 Clinical Trial.
Cited by
-
Prognostic Value of Depressive Symptoms for Cardiovascular Events in Female Patients With Heart Failure With Reduced Ejection Fraction and Heart Failure With Preserved Ejection Fraction.J Am Heart Assoc. 2024 May 7;13(9):e032961. doi: 10.1161/JAHA.123.032961. Epub 2024 Apr 30. J Am Heart Assoc. 2024. PMID: 38686893 Free PMC article.
-
Demoralization in acute coronary syndrome: Treatment and predictive factors associated with its persistence.Int J Clin Health Psychol. 2024 Jan-Mar;24(1):100444. doi: 10.1016/j.ijchp.2024.100444. Epub 2024 Jan 27. Int J Clin Health Psychol. 2024. PMID: 38317782 Free PMC article.
-
Changes over time in patient-reported outcomes in patients with heart failure.ESC Heart Fail. 2024 Apr;11(2):811-818. doi: 10.1002/ehf2.14648. Epub 2023 Dec 29. ESC Heart Fail. 2024. PMID: 38158757 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
