

Deep Intronic FGF14 GAA Repeat Expansion in Late-Onset Cerebellar Ataxia
- PMID: 36516086
- PMCID: PMC10042577
- DOI: 10.1056/NEJMoa2207406
Deep Intronic FGF14 GAA Repeat Expansion in Late-Onset Cerebellar Ataxia
Abstract
Background: The late-onset cerebellar ataxias (LOCAs) have largely resisted molecular diagnosis.
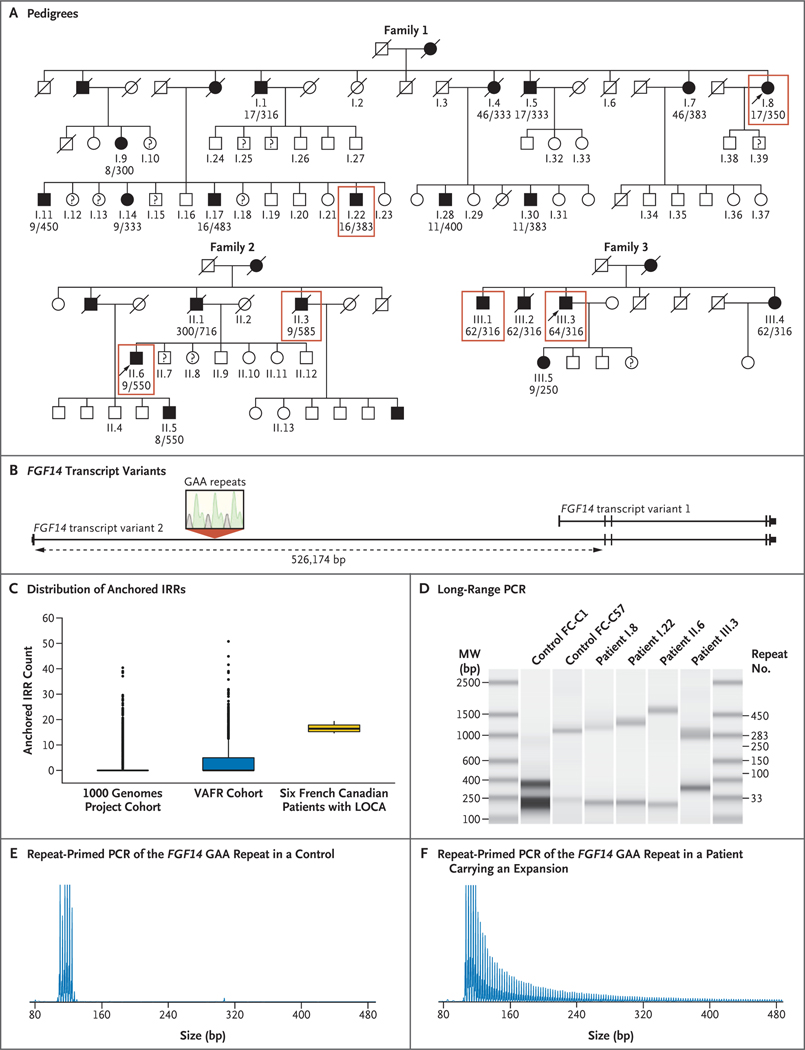
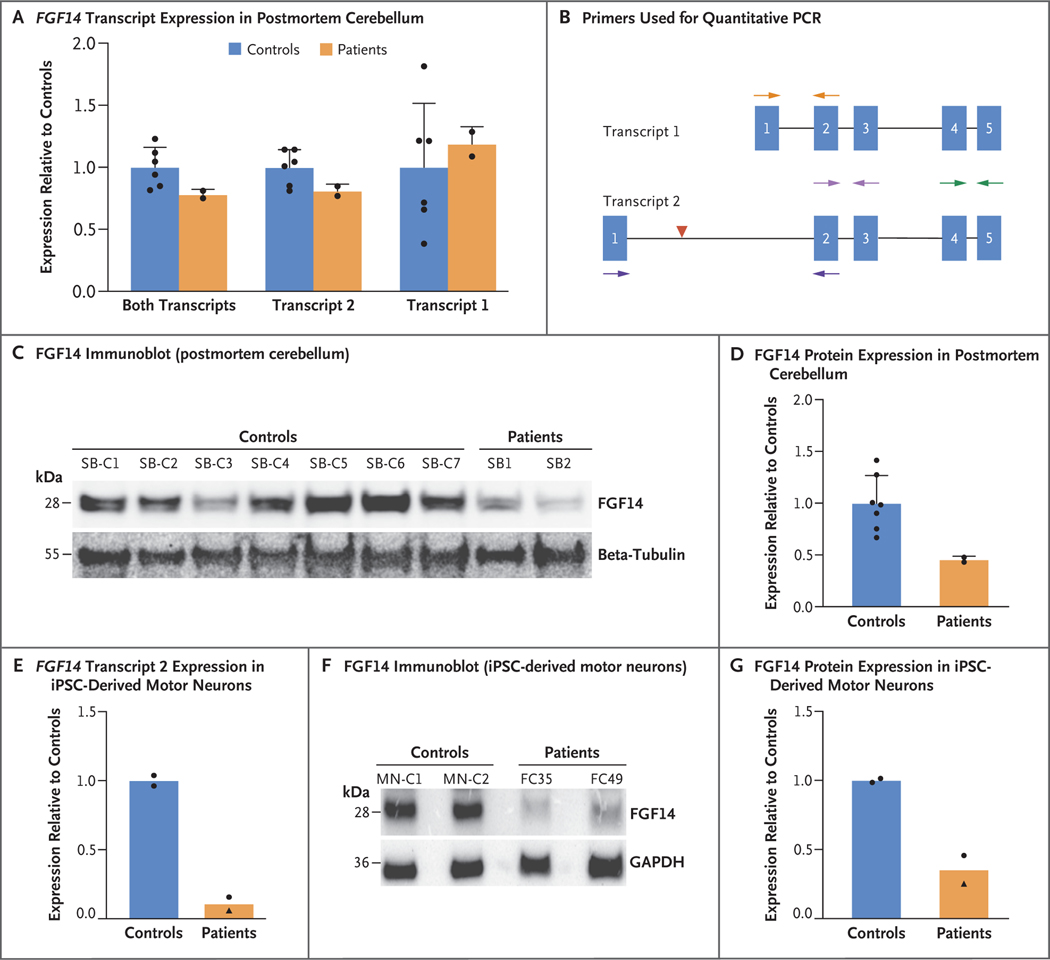
Methods: We sequenced the genomes of six persons with autosomal dominant LOCA who were members of three French Canadian families and identified a candidate pathogenic repeat expansion. We then tested for association between the repeat expansion and disease in two independent case-control series - one French Canadian (66 patients and 209 controls) and the other German (228 patients and 199 controls). We also genotyped the repeat in 20 Australian and 31 Indian index patients. We assayed gene and protein expression in two postmortem cerebellum specimens and two induced pluripotent stem-cell (iPSC)-derived motor-neuron cell lines.
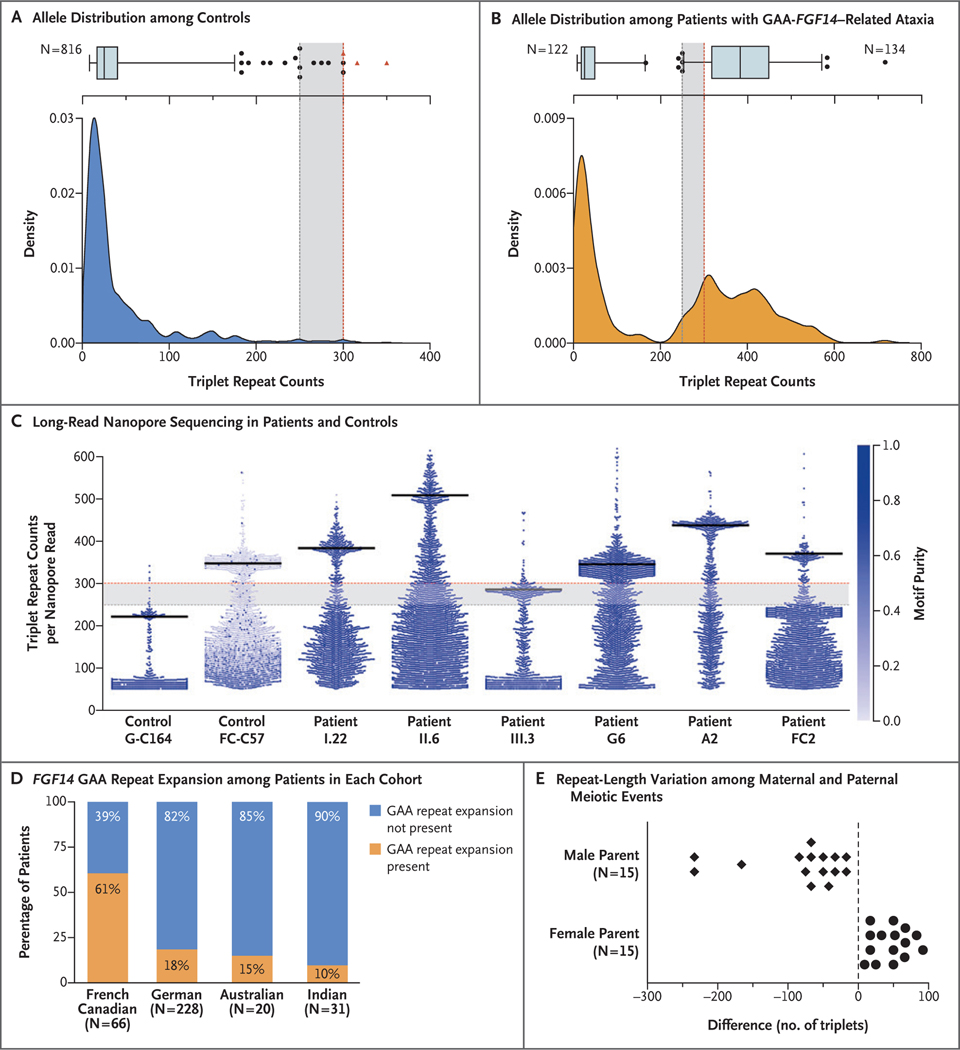
Results: In the six French Canadian patients, we identified a GAA repeat expansion deep in the first intron of FGF14, which encodes fibroblast growth factor 14. Cosegregation of the repeat expansion with disease in the families supported a pathogenic threshold of at least 250 GAA repeats ([GAA]≥250). There was significant association between FGF14 (GAA)≥250 expansions and LOCA in the French Canadian series (odds ratio, 105.60; 95% confidence interval [CI], 31.09 to 334.20; P<0.001) and in the German series (odds ratio, 8.76; 95% CI, 3.45 to 20.84; P<0.001). The repeat expansion was present in 61%, 18%, 15%, and 10% of French Canadian, German, Australian, and Indian index patients, respectively. In total, we identified 128 patients with LOCA who carried an FGF14 (GAA)≥250 expansion. Postmortem cerebellum specimens and iPSC-derived motor neurons from patients showed reduced expression of FGF14 RNA and protein.
Conclusions: A dominantly inherited deep intronic GAA repeat expansion in FGF14 was found to be associated with LOCA. (Funded by Fondation Groupe Monaco and others.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
Unraveling the Missing Heritability in Late-Onset Cerebellar Ataxia.Mov Disord. 2023 Jun;38(6):957-958. doi: 10.1002/mds.29437. Epub 2023 May 8. Mov Disord. 2023. PMID: 37157870 No abstract available.
-
Deep Intronic FGF14 GAA Repeat Expansion in Late-Onset Cerebellar Ataxia.N Engl J Med. 2023 May 25;388(21):e70. doi: 10.1056/NEJMc2301605. N Engl J Med. 2023. PMID: 37224214 No abstract available.
-
Deep Intronic FGF14 GAA Repeat Expansion in Late-Onset Cerebellar Ataxia.N Engl J Med. 2023 May 25;388(21):e70. doi: 10.1056/NEJMc2301605. N Engl J Med. 2023. PMID: 37224215 No abstract available.
-
Deep Intronic FGF14 GAA Repeat Expansion in Late-Onset Cerebellar Ataxia. Reply.N Engl J Med. 2023 May 25;388(21):e70. doi: 10.1056/NEJMc2301605. N Engl J Med. 2023. PMID: 37224216 No abstract available.
References
-
- Harding AE. “Idiopathic” late onset cerebellar ataxia: a clinical and genetic study of 36 cases. J Neurol Sci 1981; 51: 259–71. - PubMed
-
- Ruano L, Melo C, Silva MC, Coutinho P. The global epidemiology of hereditary ataxia and spastic paraplegia: a systematic review of prevalence studies. Neuroepidemiology 2014; 42: 174–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous