

A Mycobacterium tuberculosis fingerprint in human breath allows tuberculosis detection
- PMID: 36517492
- PMCID: PMC9751131
- DOI: 10.1038/s41467-022-35453-5
A Mycobacterium tuberculosis fingerprint in human breath allows tuberculosis detection
Abstract
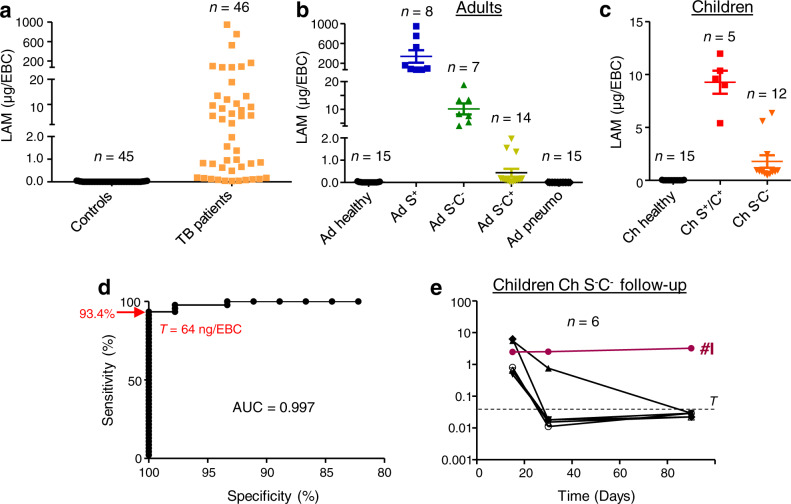
An estimated one-third of tuberculosis (TB) cases go undiagnosed or unreported. Sputum samples, widely used for TB diagnosis, are inefficient at detecting infection in children and paucibacillary patients. Indeed, developing point-of-care biomarker-based diagnostics that are not sputum-based is a major priority for the WHO. Here, in a proof-of-concept study, we tested whether pulmonary TB can be detected by analyzing patient exhaled breath condensate (EBC) samples. We find that the presence of Mycobacterium tuberculosis (Mtb)-specific lipids, lipoarabinomannan lipoglycan, and proteins in EBCs can efficiently differentiate baseline TB patients from controls. We used EBCs to track the longitudinal effects of antibiotic treatment in pediatric TB patients. In addition, Mtb lipoarabinomannan and lipids were structurally distinct in EBCs compared to ex vivo cultured bacteria, revealing specific metabolic and biochemical states of Mtb in the human lung. This provides essential information for the rational development or improvement of diagnostic antibodies, vaccines and therapeutic drugs. Our data collectively indicate that EBC analysis can potentially facilitate clinical diagnosis of TB across patient populations and monitor treatment efficacy. This affordable, rapid and non-invasive approach seems superior to sputum assays and has the potential to be implemented at point-of-care.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- WHO. Global Tuberculosis Report 2021. 1–43 (WHO, 2021).
-
- WHO. Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015. 1–3 (WHO, 2014).
-
- WHO. High-priority Target Product Profiles for New Tuberculosis Diagnostics: Report of A Consensus Meeting. 1–97 (WHO, 2014).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
