

Perioperative outcomes of robotic versus laparoscopic distal gastrectomy for gastric cancer: a meta-analysis of propensity score-matched studies and randomized controlled trials
- PMID: 36517776
- PMCID: PMC9749346
- DOI: 10.1186/s12893-022-01881-9
Perioperative outcomes of robotic versus laparoscopic distal gastrectomy for gastric cancer: a meta-analysis of propensity score-matched studies and randomized controlled trials
Abstract
Background: Da Vinci robotic surgery system, a novel type of surgery, was widespread in surgical field. However, the perioperative outcomes of robotic distal gastrectomy (RDG) are still controversy, despite several observational studies and randomized controlled trials (RCT) had been reported. Therefore, we performed a meta-analysis of propensity score-matched (PSM) and RCT studies to evaluated the perioperative feasibility and safety of RDG.
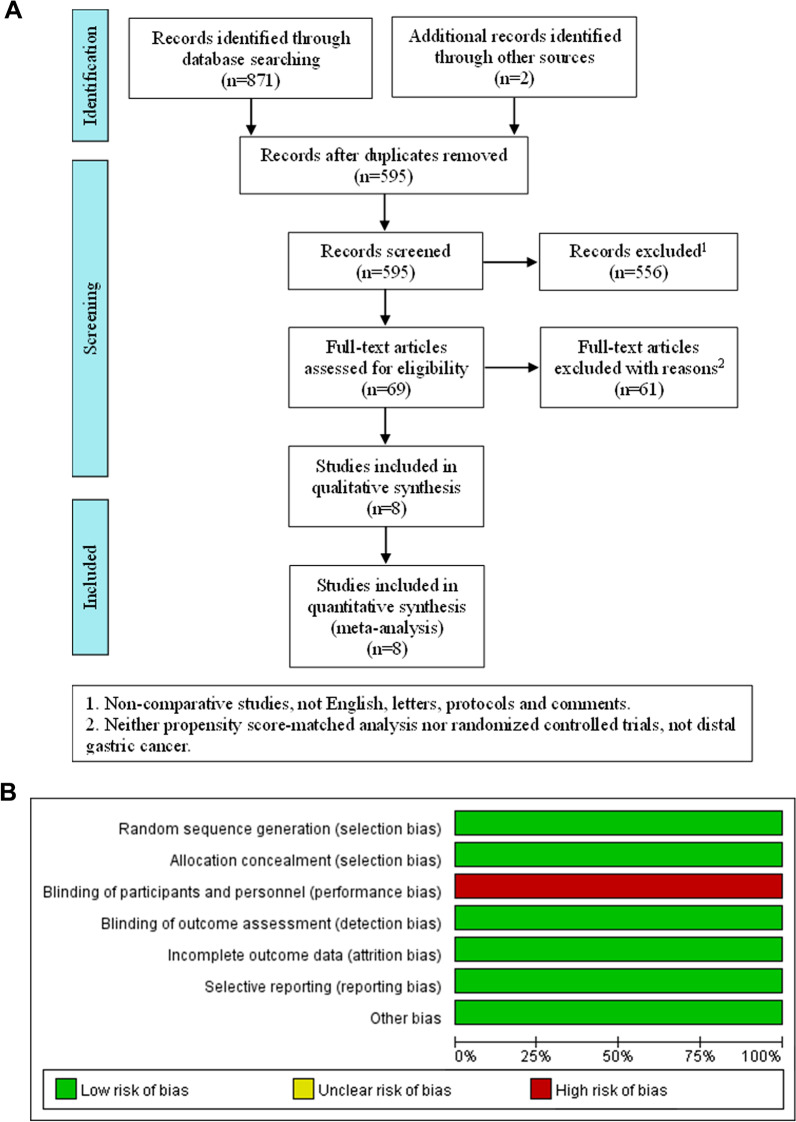
Methods: Studies were systematically searched in PubMed, Web of Science, Cochrane Library, and Embase database, and screened according to the defined limitations. The quality of PSM studies and RCT studies were respectively assessed by ROBINS-I and Cochrane risk-of-bias tool. Extracted data were analyzed by Review Manager 5.4.
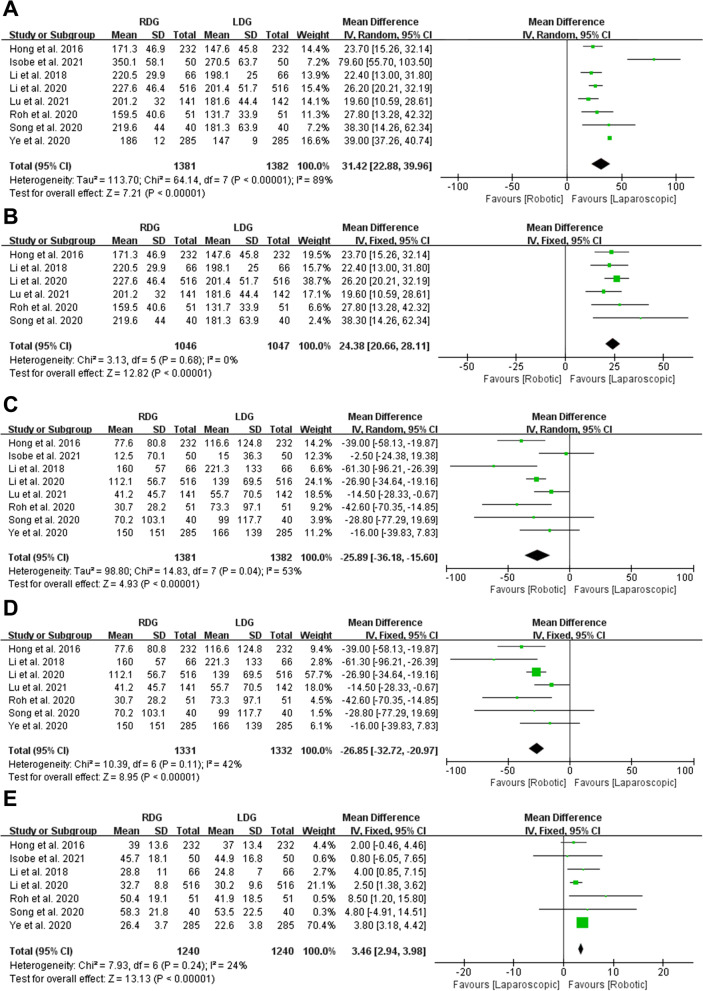
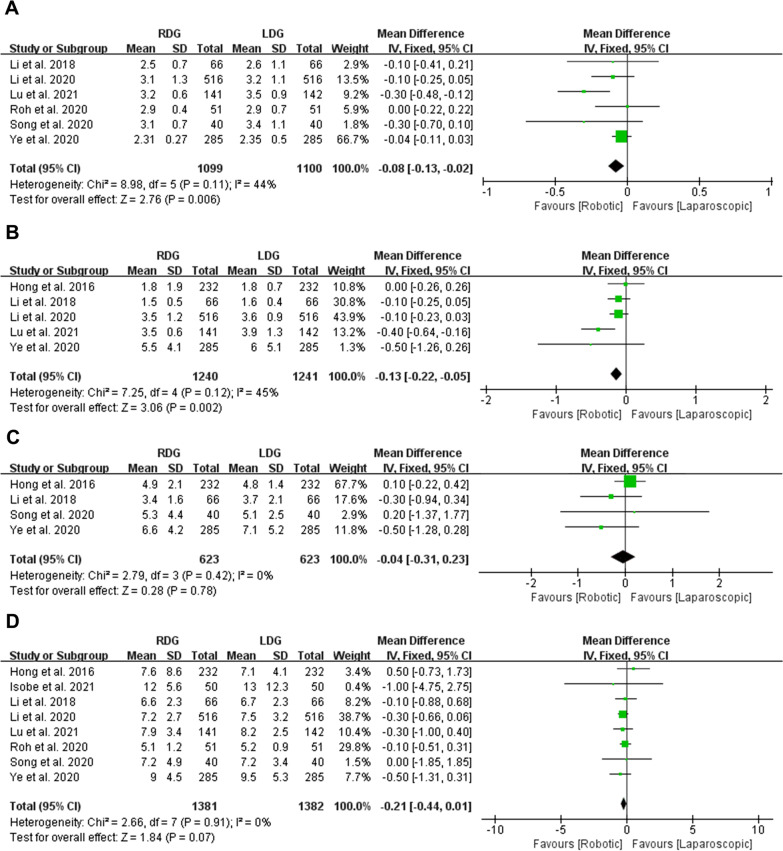
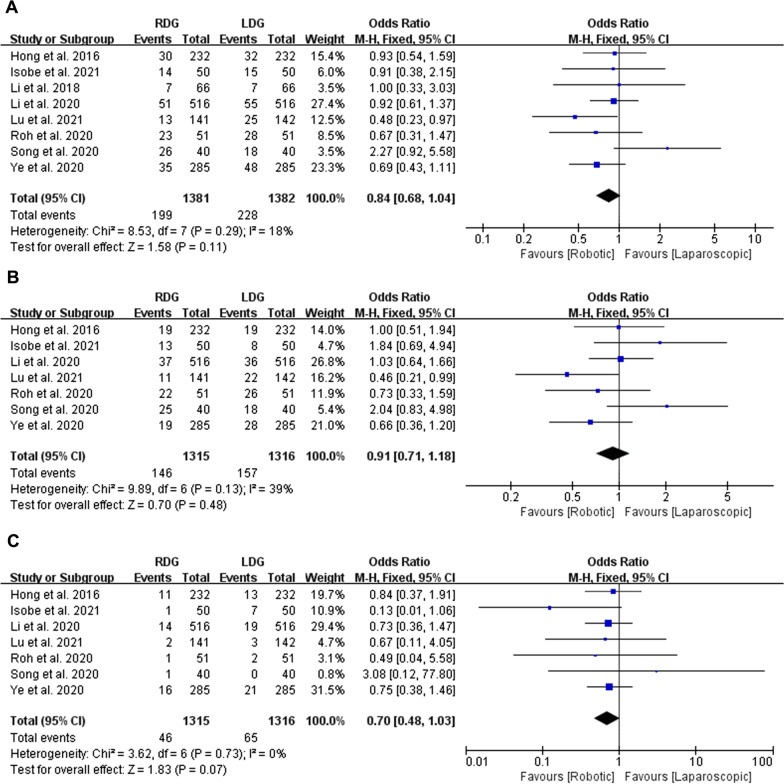
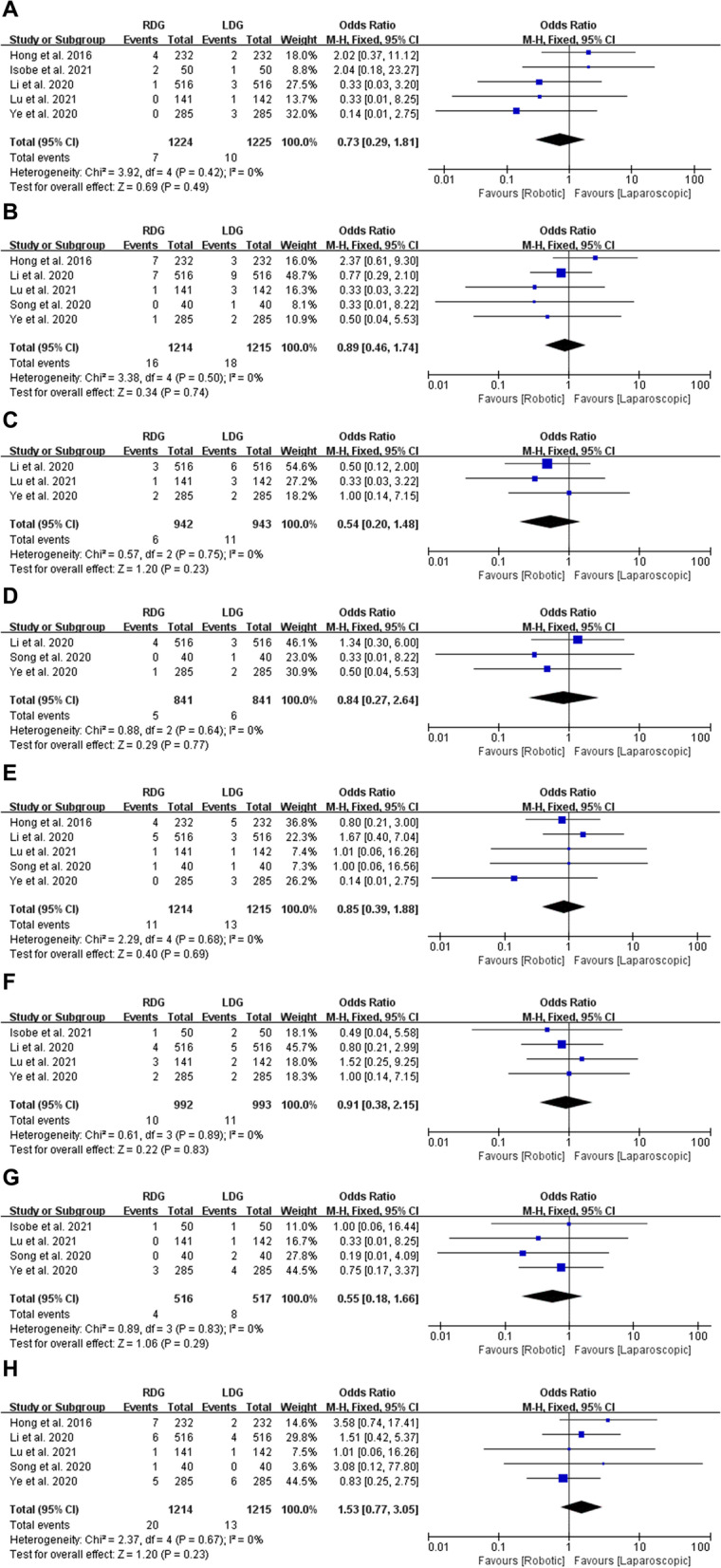
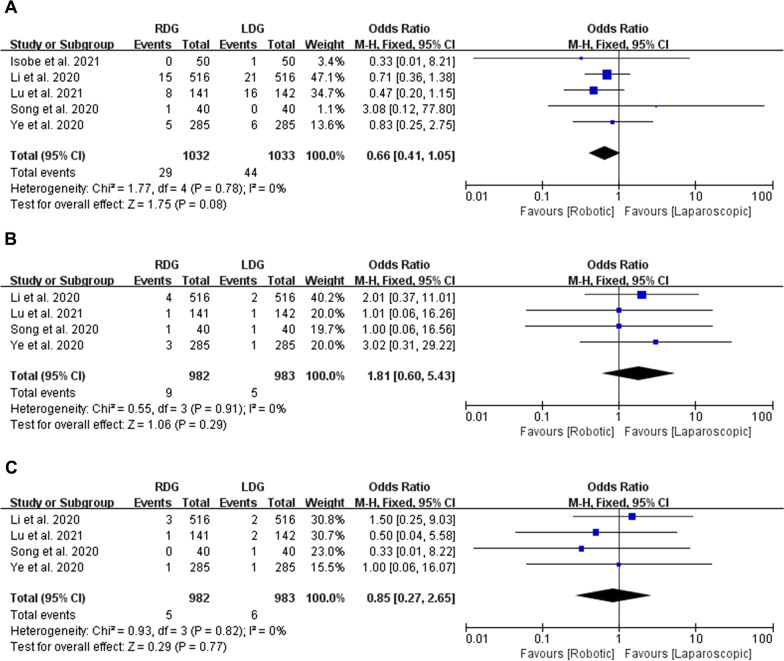
Results: 7 PSM studies and 1 RCT with a total of 2763 patients were included in this analysis. The longer operative time (MD = 31.42, 95% CI [22.88, 39.96], p < 0.00001), less blood loss (MD = - 25.89, 95% CI [- 36.18, - 15.6], p < 0.00001), more retrieved lymph nodes (MD = 3.46, 95% CI [2.94, 3.98], p < 0.00001), shorter time to first flatus (MD = - 0.08, 95% CI [- 0.13, - 0.02], p = 0.006) and liquid intake (MD = - 0.13, 95% CI [- 0.22, - 0.05], p = 0.002) were observed in RDG group compared with LDG group. There are no statistically significant in time to start soft diet, postoperative hospital stays, overall complications, complications Grade I-II, complications Grade ≥ III, anastomotic leakage, bleeding, intra-abdominal bleeding, intraluminal bleeding, ileus, abdominal infection, delayed gastric emptying and wound complications.
Conclusions: RDG showed less blood loss and more retrieved lymph nodes, revealed less time to first flatus and liquid intake after operation. But the operative time was longer in RDG group than in LDG. The incidence rate of postoperative complications was comparable between RDG and LDG.
Keywords: Gastric cancer; Laparoscopic distal gastrectomy; Meta-analysis; Robotic distal gastrectomy.
© 2022. The Author(s).
Conflict of interest statement
Authors declare no conflict of interests for this article.
Figures
References
-
- Li J, Xi H, Guo X, Gao Y, Xie T, Qiao Z, et al. Surgical outcomes and learning curve analysis of robotic gastrectomy for gastric cancer: multidimensional analysis compared with threedimensional highdefinition laparoscopic gastrectomy. Int J Oncol. 2019;55:733–744. - PubMed
-
- Furukawa T, Wakabayashi G, Ozawa S, Watanabe M, Ohgami M, Kitagawa Y, et al. Surgery using master–slave manipulators and telementoring. Nihon Geka Gakkai Zasshi. 2000;101:293–298. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
