

Hepatocellular carcinoma risk-stratification based on ASGR1 in circulating epithelial cells for cancer interception
- PMID: 36518850
- PMCID: PMC9742249
- DOI: 10.3389/fmolb.2022.1074277
Hepatocellular carcinoma risk-stratification based on ASGR1 in circulating epithelial cells for cancer interception
Abstract
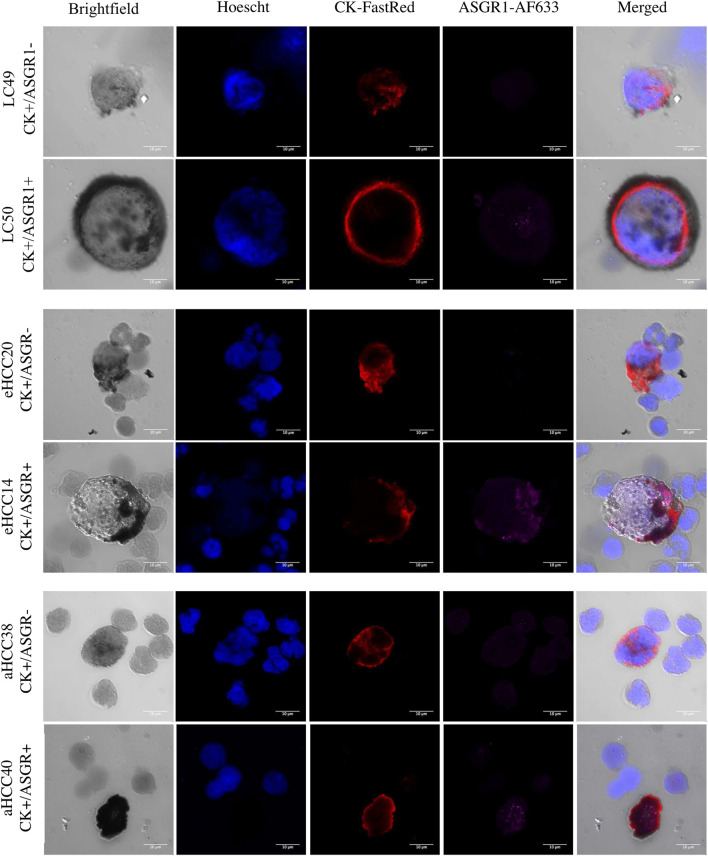
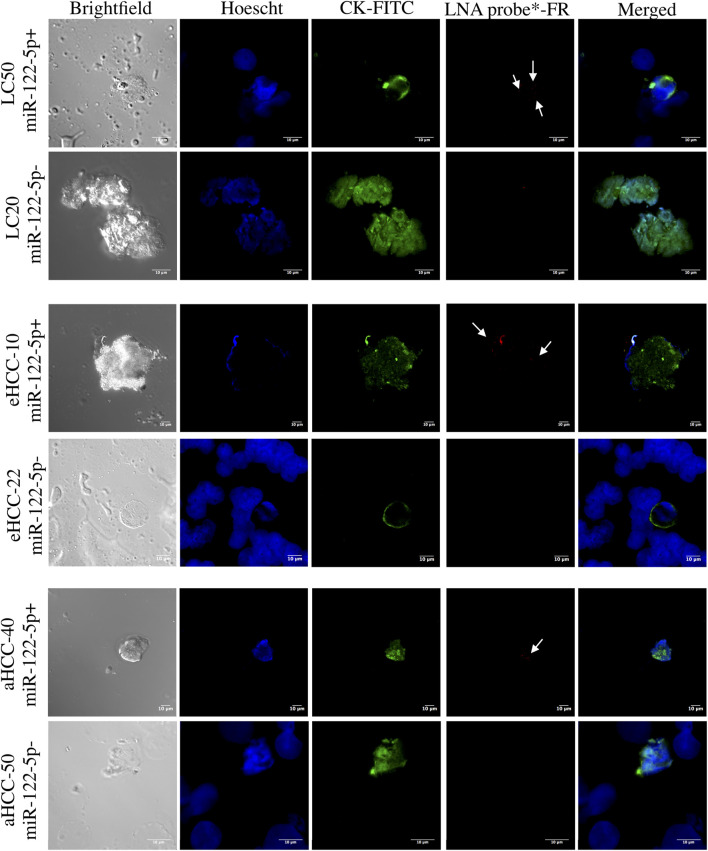
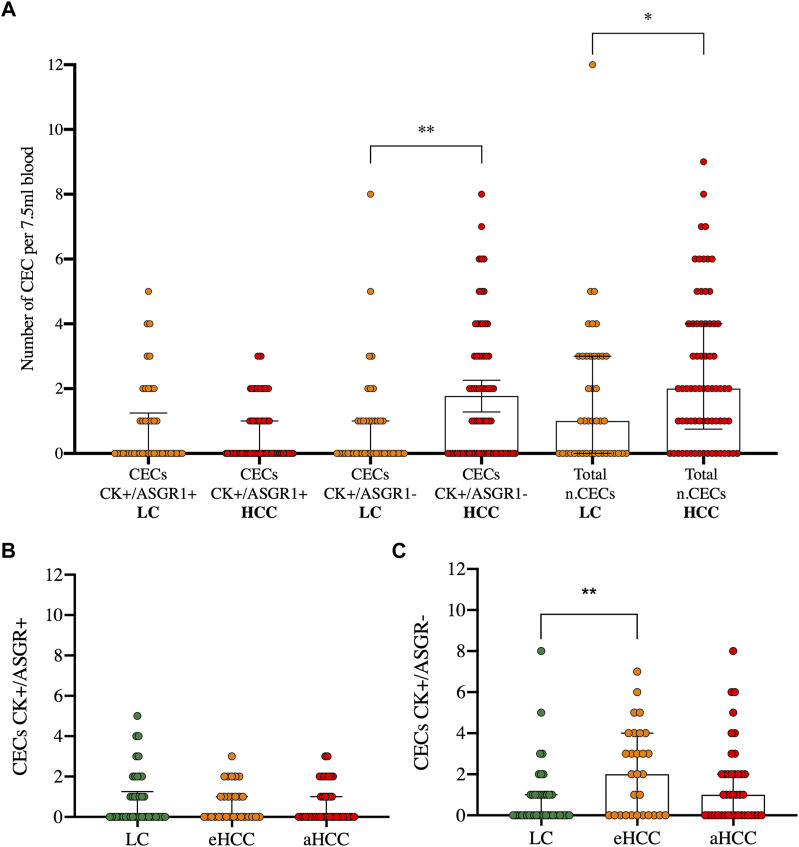
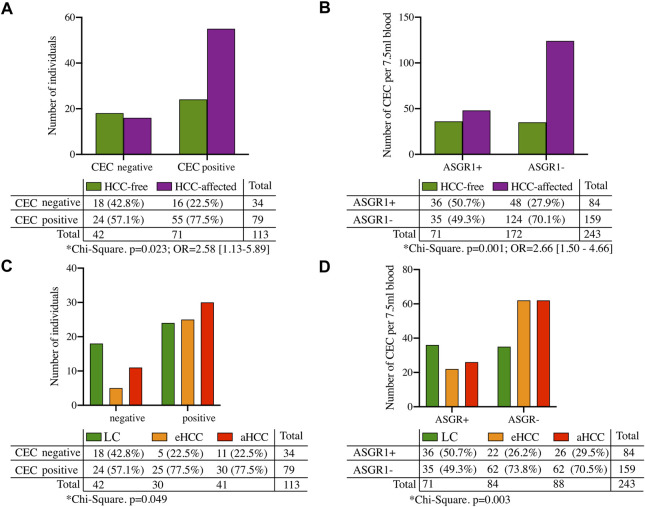
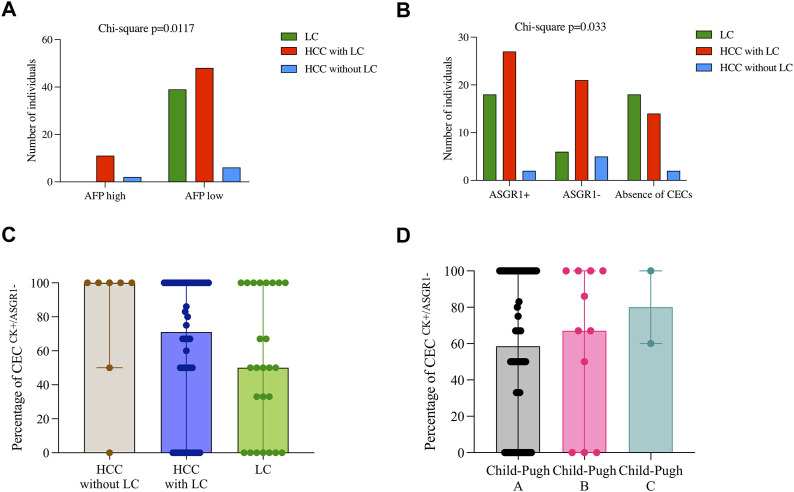
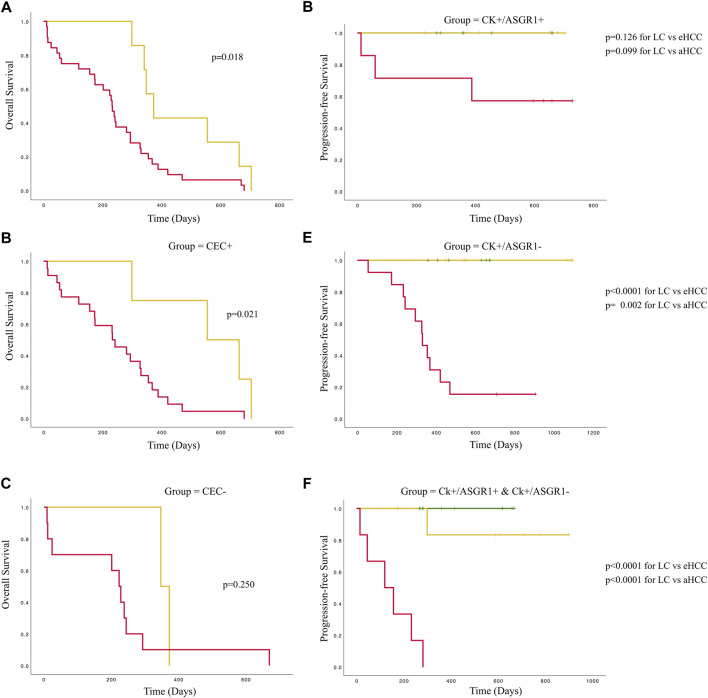
Purpose: Lack of diagnostic and prognostic biomarkers in hepatocellular carcinoma impedes stratifying patients based on their risk of developing cancer. The aim of this study was to evaluate phenotypic and genetic heterogeneity of circulating epithelial cells (CECs) based on asialoglycoprotein receptor 1 (ASGR1) and miR-122-5p expression as potential diagnostic and prognostic tools in patients with hepatocellular carcinoma (HCC) and liver cirrhosis (LC). Methods: Peripheral blood samples were extracted from LC and HCC patients at different disease stages. CECs were isolated using positive immunomagnetic selection. Genetic and phenotypic characterization was validated by double immunocytochemistry for cytokeratin (CK) and ASGR1 or by in situ hybridization with miR-122-5p and CECs were visualized by confocal microscopy. Results: The presence of CECs increased HCC risk by 2.58-fold, however, this was only significant for patients with previous LC (p = 0.028) and not for those without prior LC (p = 0.23). Furthermore, the number of CECs lacking ASGR1 expression correlated significantly with HCC incidence and absence of miR-122-5p expression (p = 0.014; r = 0.23). Finally, overall survival was significantly greater for patients at earlier cancer stages (p = 0.018), but this difference was only maintained in the group with the presence of CECs (p = 0.021) whereas progression-free survival was influenced by the absence of ASGR1 expression. Conclusion: Identification and characterization of CECs by ASGR1 and/or miR-122-5p expression may be used as a risk-stratification tool in LC patients, as it was shown to be an independent prognostic and risk-stratification marker in LC and early disease stage HCC patients.
Keywords: cancer interception; circulating tumor cells; hepatocellular carcinoma; liver cirrhosis; precision medicine.
Copyright © 2022 Roa-Colomo, López Garrido, Molina-Vallejo, Rojas, Sanchez, Aranda-García, Salmeron, Romero-Gomez, Muntane, Padillo, Alamo, Lorente, Serrano and Garrido-Navas.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bayarri-Lara C., Ortega F. G., Cueto Ladrón de Guevara A., Puche J. L., Ruiz Zafra J., de Miguel-Perez D., et al. (2016). Circulating tumor cells identify early recurrence in patients with non-small cell lung cancer undergoing radical resection. PLoS One 11, e0148659. 10.1371/journal.pone.0148659 - DOI - PMC - PubMed
-
- Cancer Tomorrow (2022). Cancer Tomorrow. Available at: https://gco.iarc.fr/tomorrow/en/dataviz/isotype?cancers=11&single_unit=5... . [Accessed 22 Sep 2022].
LinkOut - more resources
Full Text Sources
Research Materials