

Alterations in gut microbiome and metabolomics in chronic hepatitis B infection-associated liver disease and their impact on peripheral immune response
- PMID: 36519342
- PMCID: PMC9757487
- DOI: 10.1080/19490976.2022.2155018
Alterations in gut microbiome and metabolomics in chronic hepatitis B infection-associated liver disease and their impact on peripheral immune response
Abstract
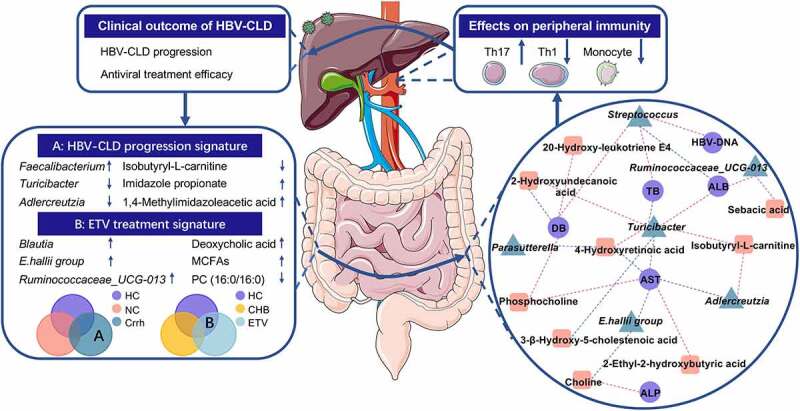
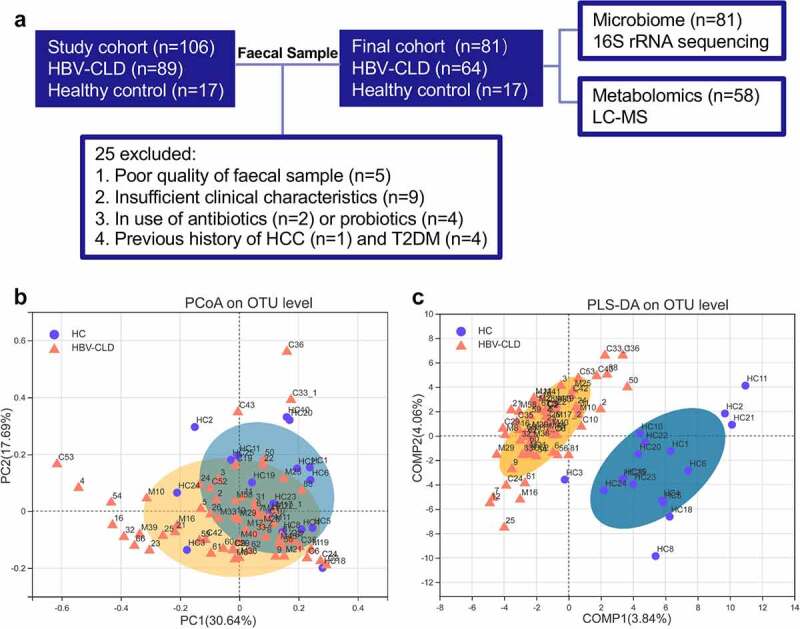
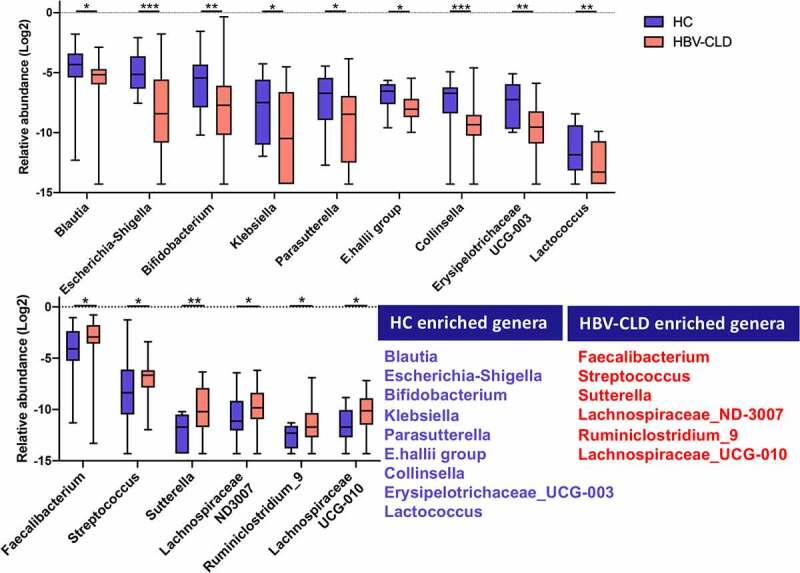
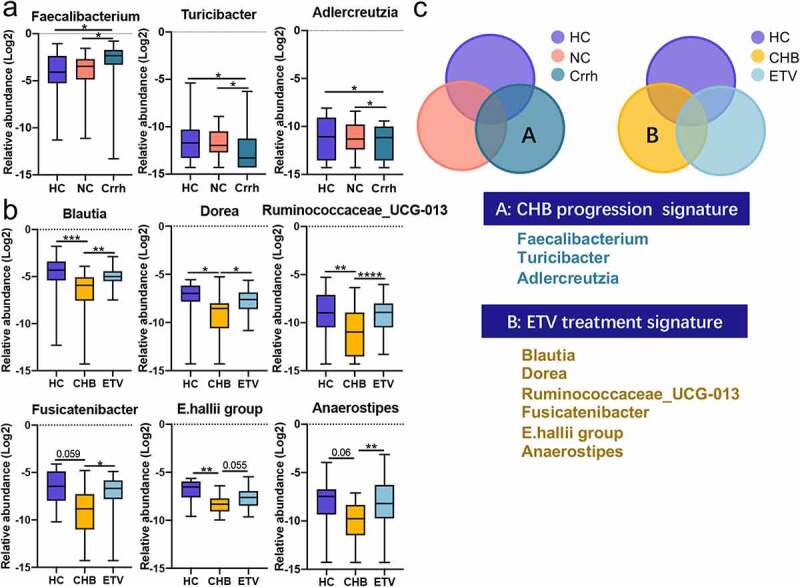
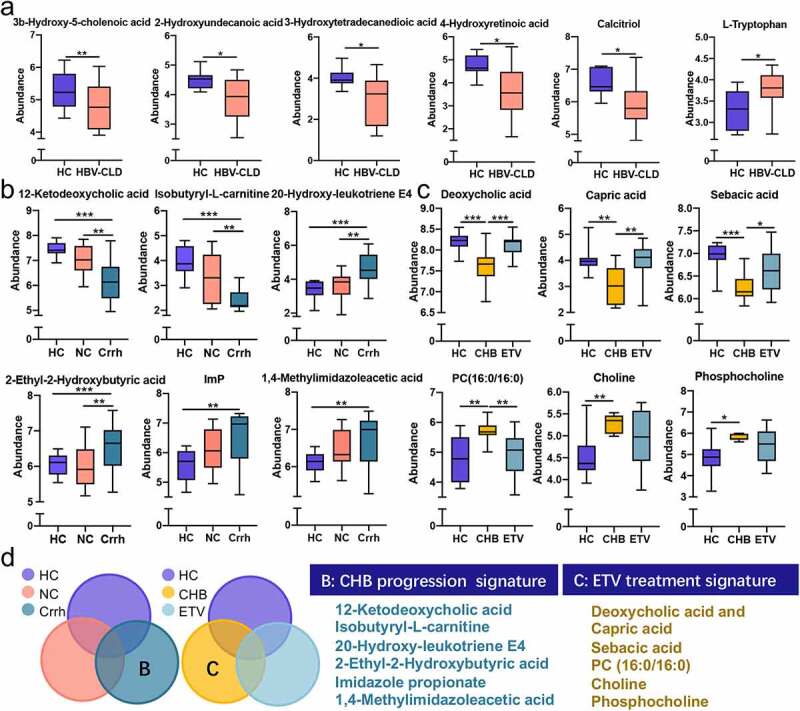
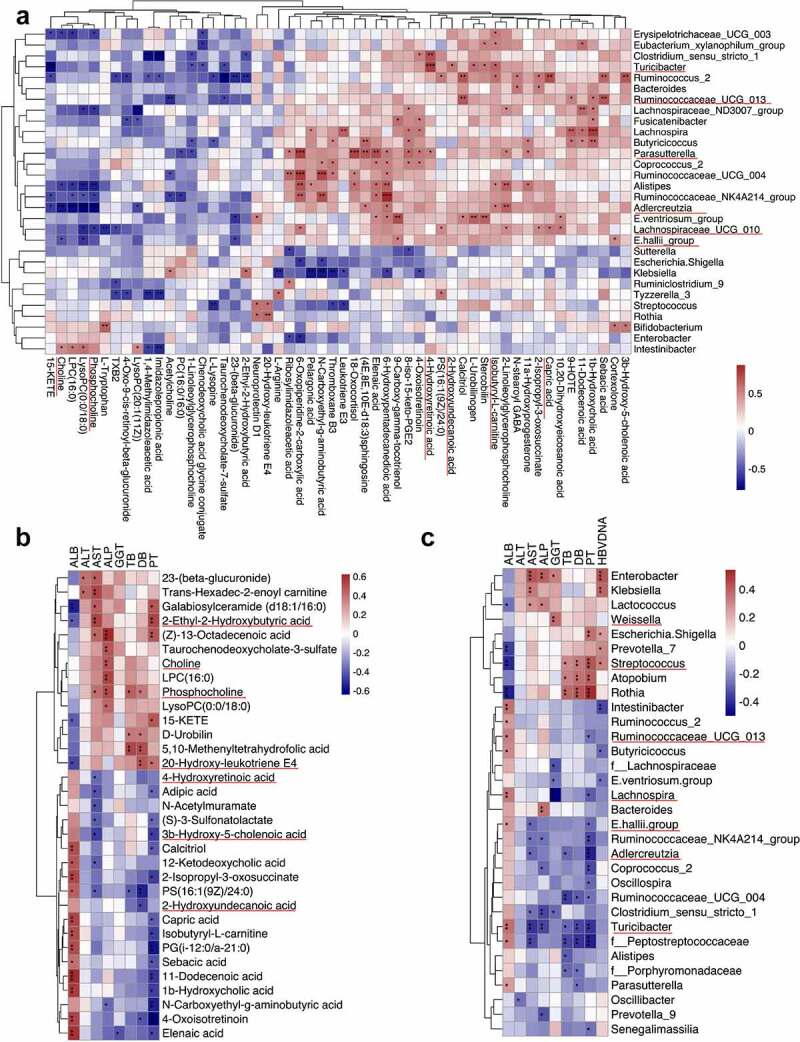
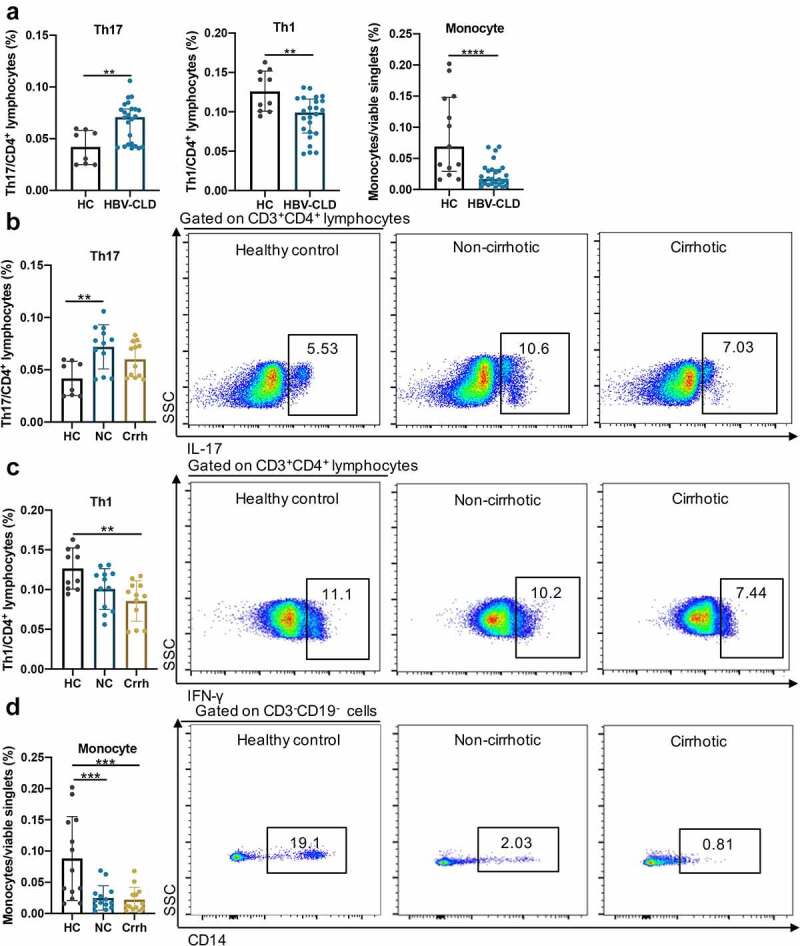
Gut dysbiosis has been reported in chronic hepatitis B (CHB) infection, however its role in CHB progression and antiviral treatment remains to be clarified. Herein, the present study aimed to characterize gut microbiota (GM) in patients with chronic hepatitis B virus infection-associated liver diseases (HBV-CLD) by combining microbiome with metabolome analyses and to evaluate their effects on peripheral immunity. Fecal samples from HBV-CLD patients (n = 64) and healthy controls (n = 17) were collected for 16s rRNA sequencing. Fecal metabolomics was measured with untargeted liquid chromatography-mass spectrometry in subgroups of 58 subjects. Lineage changes of peripheral blood mononuclear cells (PBMCs) were determined upon exposure to bacterial extracts (BE) from HBV-CLD patients. Integrated analyses of microbiome with metabolome revealed a remarkable shift of gut microbiota and metabolites in HBV-CLD patients, and disease progression and antiviral treatment were found to be two main contributing factors for the shift. Concordant decreases in Turicibacter with 4-hydroxyretinoic acid were detected to be inversely correlated with serum AST levels through host-microbiota-metabolite interaction analysis in cirrhotic patients. Moreover, depletion of E.hallii group with elevated choline was restored in patients with 5-year antiviral treatment. PBMC exposure to BE from non-cirrhotic patients enhanced expansion of T helper 17 cells; however, BE from cirrhotics attenuated T helper 1 cell count. CHB progression and antiviral treatment are two main factors contributing to the compositional shift in microbiome and metabolome of HBV-CLD patients. Peripheral immunity might be an intermediate link in gut microbe-host interplay underlying CHB pathogenesis.
Keywords: Chronic hepatitis B virus infection-associated liver disease; antiviral treatment; cirrhosis; metabolome; microbiome; peripheral immunity.
Plain language summary
Integrated analyses of microbiome with metabolomics revealed a remarkable shift of gut microbiota and metabolites in HBV-CLD patients. Disease progression and entecavir treatment were found to be two main contributing factors for the shift. Novel host-microbiota-metabolite interplay was investigated (red, positive correlation; blue, negative correlation). Ex vivo results showed that exposure of PBMCs to BE from non-cirrhotic patients promoted expansion of T helper 17 cells whilst BE from cirrhotic patients attenuated T helper 1 cell count, suggesting peripheral immunity may be one of mechanisms by which overall bacterial products exert profibrotic effects and have an impact on prognosis of HBV-CLD patients. Our research confers new insights into the role of gut dysbiosis and metabolomics in the pathogenesis of HBV-CLD, and underscores that disrupted peripheral immunity homeostasis during the microbe-host interplay may contribute to fibrosis progression in HBV-CLD. CHB, chronic hepatitis B (treatment-naive); Crrh, cirrhosis; ETV, entecavir; HBV-CLD, chronic hepatitis B virus infection-associated liver diseases; HCs, healthy controls; MCFAs, medium chain fatty acids; NC, non-cirrhosis; Th1, T helper 1; Th17, T helper 17.Abbreviations: ALB, albumin; ALP, alkaline phosphatase; ANOISM, analysis of similarities; AST, aspartate aminotransferase; BE, bacterial extracts; BMI, body mass index; CC, compensated cirrhosis; CHB, chronic hepatitis B; DB, direct bilirubin; DC, decompensated cirrhosis; DCA, deoxycholic acid; ETV, entecavir; FDR, false discovery rate; GGT, γ-glutamyl transpeptidase; GM, gut microbiota; HBV, hepatitis B virus; HBV-CLD, chronic hepatitis B virus infection-associated liver diseases; HCs, healthy controls; HCC, hepatocellular carcinoma; LC-MS, liquid chromatography-mass spectrometry; LRE, liver-related events; LS, liver stiffness; ImP, imidazole propionate; IQR, interquartile range; MCFAs, medium chain fatty acids; OCT, organic cation transporter; OPLS-DA, orthogonal partial least square discriminant analysis; PBMCs, peripheral blood mononuclear cells; PERMANOVA, permutational multivariate analysis of variance; PLS-DA, partial least square discriminant analysis; PCA, principal component analysis; PcoA, principal coordinates analysis; PT, prolonged prothrombin time; SDs, standard deviations; TB, total bilirubin; Tregs, regulatory T cells; Th1, T helper 1; Th17, T helper 17.
Conflict of interest statement
All authors declare that no conflict of interest is associated with participation and contribution to this work.
Figures
References
-
- Polaris Observatory C, Gamkrelidze I, Nguyen MH, Chen D-S, Van Damme P, Abbas Z, Abdulla M, Abou Rached A, Adda D, Aho I. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. 2018;3:383–403. doi:10.1016/S2468-1253(18)30056-6. - DOI - PubMed
-
- Lampertico P, Agarwal K, Berg T, Buti M, Janssen HLA, Papatheodoridis G, Zoulim F, Tacke F. European Association for the Study of the Liver . Electronic address eee, European association for the study of the L. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous