A thickened formula reduces feeding-associated oxygen desaturation and bradycardia in preterm infants
- PMID: 36521453
- PMCID: PMC9815936
- DOI: 10.3345/cep.2022.00780
A thickened formula reduces feeding-associated oxygen desaturation and bradycardia in preterm infants
Abstract
Background: Although preterm infants often experience desaturation or bradycardia during oral feeding, specific guidelines for its management are lacking.
Purpose: This study aimed to investigate the effects of a commercial thickened formula (TF) on oxygen saturation and heart rate stabilization during oral feeding in preterm infants.
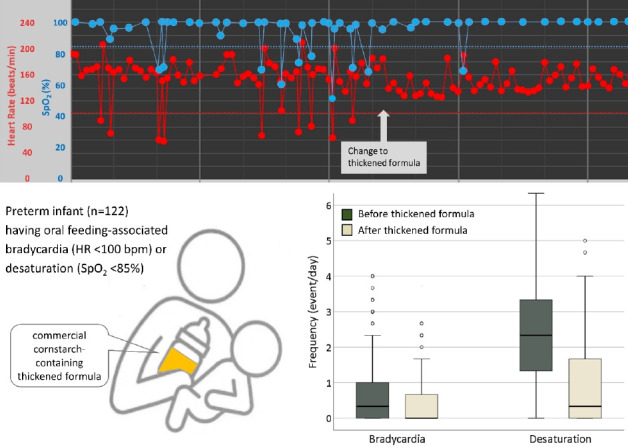
Methods: This retrospective study included 122 infants born at a median (interquartile range [IQR]) 31+6 weeks (29+4 -34+6 weeks) of gestation weighing 1,725 g (1,353-2,620 g) and fed commercial cornstarch-containing TF due to feeding-associated desaturation or bradycardia. We excluded infants fed TF to treat symptomatic regurgitation. Desaturation and bradycardia events were compared between 3 days prior to the change and 3 days after the change to TF. Desaturation and bradycardia were defined as SpO2 <85% and heart rate <100 beats/min during or immediately after oral bottle feeding, respectively.
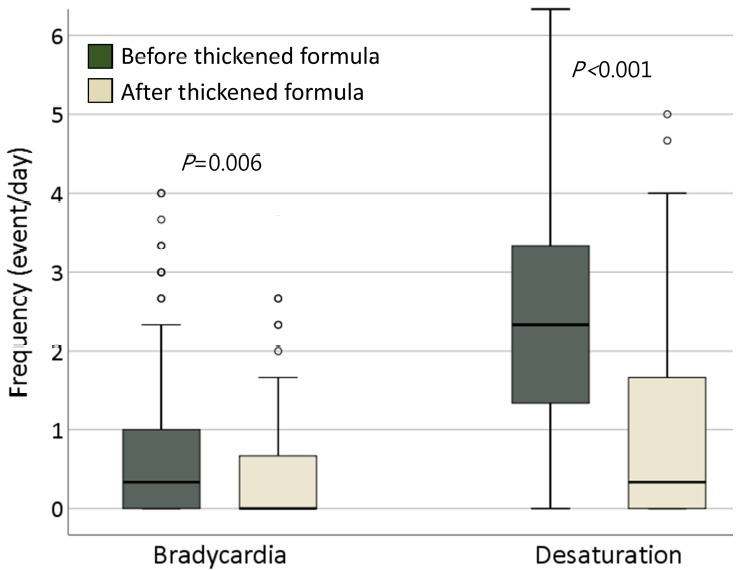
Results: The median (IQR) postmenstrual age and weight were 36+1 weeks (34+6-38+0 weeks) and 2,395 g (2,160-2,780 g), respectively, at the time of change to TF. The frequency of desaturation significantly decreased after TF feeding (median [IQR]: 2.3 [1.3-3.3] events/day vs. 0.3 [0-1.7] events/day, P< 0.001). Bradycardia also decreased after TF feeding (0.3 [0-1] events/day vs. 0 [0-0.7] events/day, P=0.006). There were no cases of diarrhea or electrolyte abnormalities after TF feeding. Defecation frequency decreased (P=0.037), and polyethylene glycol was prescribed to 27% of the TF-fed infants. In a subgroup analysis of 16 infants with bronchopulmonary dysplasia, the frequency of desaturation was reduced (2.3 [1.8-3.8] events/day vs. 0.5 [0-1.5] events/day, P=0.042), and weight gain improved (22.5 [3.1-36.3] g/day vs. 41.3 [28.1-55.1] g/day, P=0.019), after TF feeding.
Conclusion: TF feeding significantly reduces oral feeding-associated oxygen desaturation and bradycardia in preterm infants. TF may be useful for stabilizing oxygen saturation and heart rate among preterm infants with difficulties in oral feeding.
Keywords: Bottle feeding; Feeding behavior; Infant nutritional physiological phenomena; Thickened.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Motion S, Northstone K, Emond A. Persistent early feeding difficulties and subsequent growth and developmental outcomes. Ambul Child Heal. 2001;7:231–7.
-
- Eichenwald EC, Blackwell M, Lloyd JS, Tran T, Wilker RE, Richardson DK. Inter-neonatal intensive care unit variation in discharge timing: Influence of apnea and feeding management. Pediatrics. 2001;108:928–33. - PubMed
-
- Rommel N, De Meyer AM, Feenstra L, Veereman-Wauters G. The complexity of feeding problems in 700 infants and young children presenting to a tertiary care institution. J Pediatr Gastroenterol Nutr. 2003;37:75–84. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous