

Characteristics, therapies, and outcomes of In-Hospital vs Out-of-Hospital cardiac arrest in patients presenting to cardiac intensive care units: From the critical care Cardiology trials network (CCCTN)
- PMID: 36521683
- PMCID: PMC9899313
- DOI: 10.1016/j.resuscitation.2022.12.002
Characteristics, therapies, and outcomes of In-Hospital vs Out-of-Hospital cardiac arrest in patients presenting to cardiac intensive care units: From the critical care Cardiology trials network (CCCTN)
Abstract
Background: Cardiac arrest (CA) is a common reason for admission to the cardiac intensive care unit (CICU), though the relative burden of morbidity, mortality, and resource use between admissions with in-hospital (IH) and out-of-hospital (OH) CA is unknown. We compared characteristics, care patterns, and outcomes of admissions to contemporary CICUs after IHCA or OHCA.
Methods: The Critical Care Cardiology Trials Network is a multicenter network of tertiary CICUs in the US and Canada. Participating centers contributed data from consecutive admissions during 2-month annual snapshots from 2017 to 2021. We analyzed characteristics and outcomes of admissions by IHCA vs OHCA.
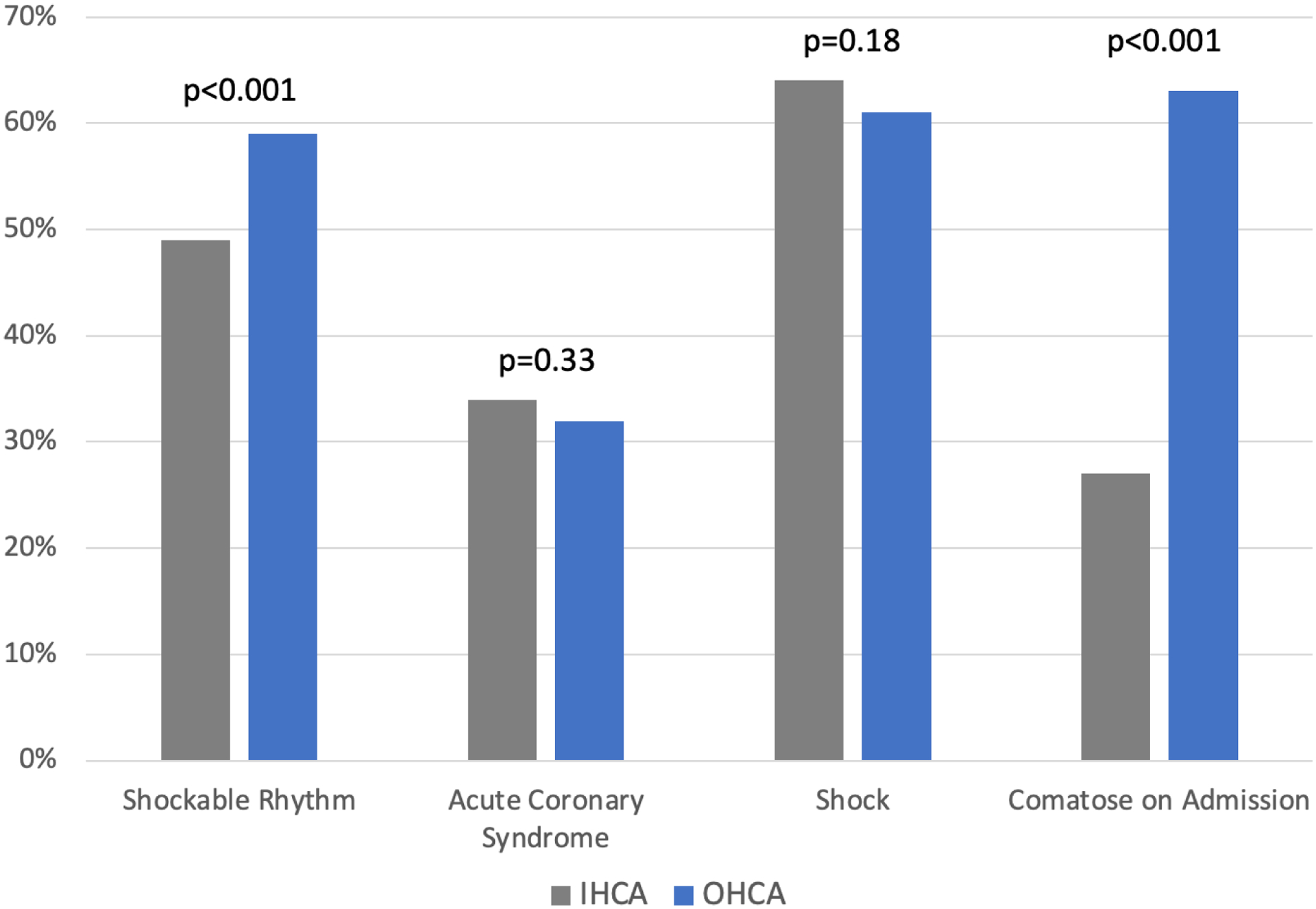
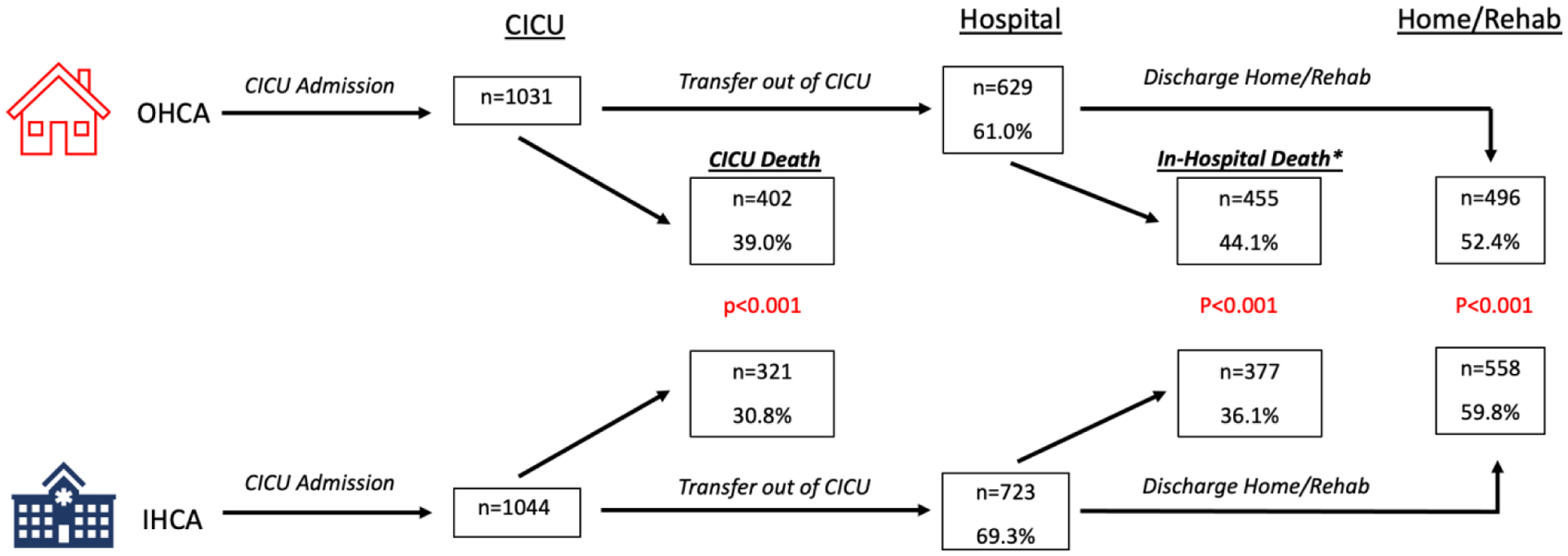
Results: We analyzed 2,075 admissions across 29 centers (50.3% IHCA, 49.7% OHCA). Admissions with IHCA were older (median 66 vs 62 years), more commonly had coronary disease (38.3% vs 29.7%), atrial fibrillation (26.7% vs 15.6%), and heart failure (36.3% vs 22.1%), and were less commonly comatose on CICU arrival (34.2% vs 71.7%), p < 0.001 for all. IHCA admissions had lower lactate (median 4.3 vs 5.9) but greater utilization of invasive hemodynamics (34.3% vs 23.6%), mechanical circulatory support (28.4% vs 16.8%), and renal replacement therapy (15.5% vs 9.4%); p < 0.001 for all. Comatose IHCA patients underwent targeted temperature management less frequently than OHCA patients (63.3% vs 84.9%, p < 0.001). IHCA admissions had lower unadjusted CICU (30.8% vs 39.0%, p < 0.001) and in-hospital mortality (36.1% vs 44.1%, p < 0.001).
Conclusion: Despite a greater burden of comorbidities, CICU admissions after IHCA have lower lactate, greater invasive therapy utilization, and lower crude mortality than admissions after OHCA.
Keywords: CICU; Cardiac arrest; IHCA; OHCA; TTM; cardiac critical care; cardiac intensive care unit; in-hospital cardiac arrest; out-of-hospital cardiac arrest; targeted temperature management.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Bohula EA, Katz JN, van Diepen S, Alviar CL, Baird-Zars VM, Park JG, et al. Demographics, Care Patterns, and Outcomes of Patients Admitted to Cardiac Intensive Care Units: The Critical Care Cardiology Trials Network Prospective North American Multicenter Registry of Cardiac Critical Illness. JAMA Cardiol. 2019;4:928–35. - PMC - PubMed
-
- Fugate JE, Brinjikji W, Mandrekar JN, Cloft HJ, White RD, Wijdicks EF, et al. Post-cardiac arrest mortality is declining: a study of the US National Inpatient Sample 2001 to 2009. Circulation. 2012;126:546–50. - PubMed
-
- Radeschi G, Mina A, Berta G, Fassiola A, Roasio A, Urso F, et al. Incidence and outcome of in-hospital cardiac arrest in Italy: a multicentre observational study in the Piedmont Region. Resuscitation. 2017;119:48–55. - PubMed
-
- Nolan JP, Soar J, Smith GB, Gwinnutt C, Parrott F, Power S, et al. Incidence and outcome of in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation. 2014;85:987–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
