

Spinal Cord Ischemia in Open and Endovascular Aortic Repair
- PMID: 36521813
- PMCID: PMC9754877
- DOI: 10.1055/s-0042-1756669
Spinal Cord Ischemia in Open and Endovascular Aortic Repair
Abstract
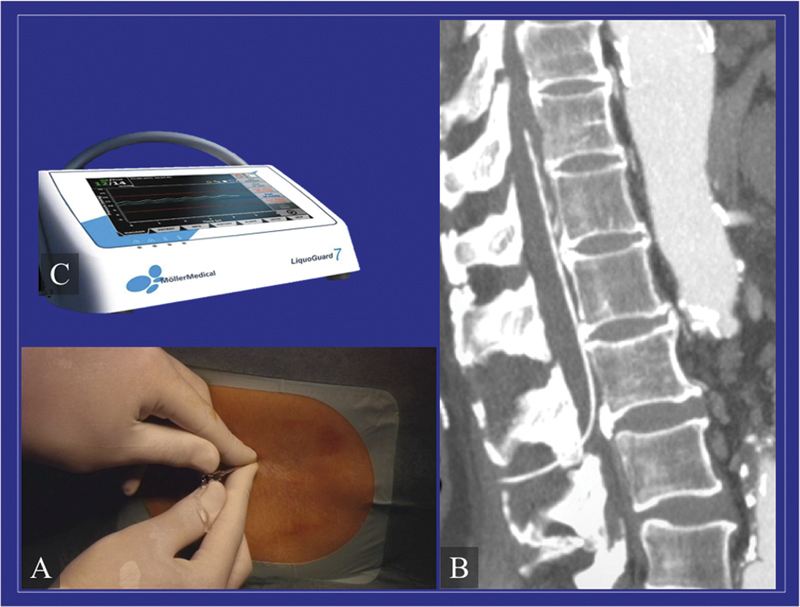
Despite the improvements, spinal cord ischemia is still one of the major and most dramatic potential complications after thoracic and thoracoabdominal aortic treatments, for both open and endovascular procedures. A multimodal approach, which includes several intraoperative and postoperative maneuvers, may contribute to optimizing the spinal cord tolerance to ischemia. The aim of this article is to report the different techniques employed to improve spinal cord perfusion, directly and indirectly through collateral circulation.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
The authors declare no conflict of interest related to this article.
Figures
References
-
- Kouchoukos N T, Kulik A, Castner C F.Outcomes after thoracoabdominal aortic aneurysm repair using hypothermic circulatory arrest J Thorac Cardiovasc Surg 2013145(3, suppl):S139–S141. - PubMed
-
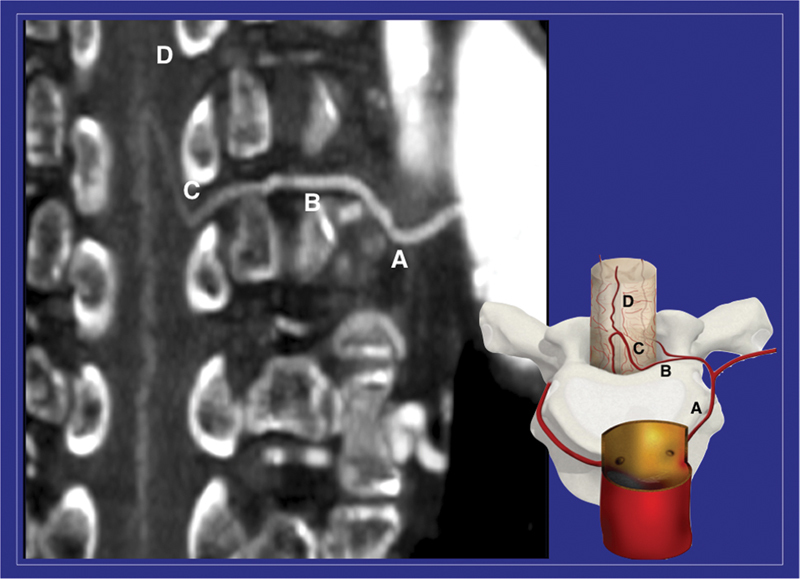
- Melissano G, Bertoglio L, Rinaldi E, Leopardi M, Chiesa R. An anatomical review of spinal cord blood supply. J Cardiovasc Surg (Torino) 2015;56(05):699–706. - PubMed
-
- Griepp R B, Griepp E B.Spinal cord perfusion and protection during descending thoracic and thoracoabdominal aortic surgery: the collateral network concept Ann Thorac Surg 20078302S865–S869., discussion S890–S892 - PubMed
-
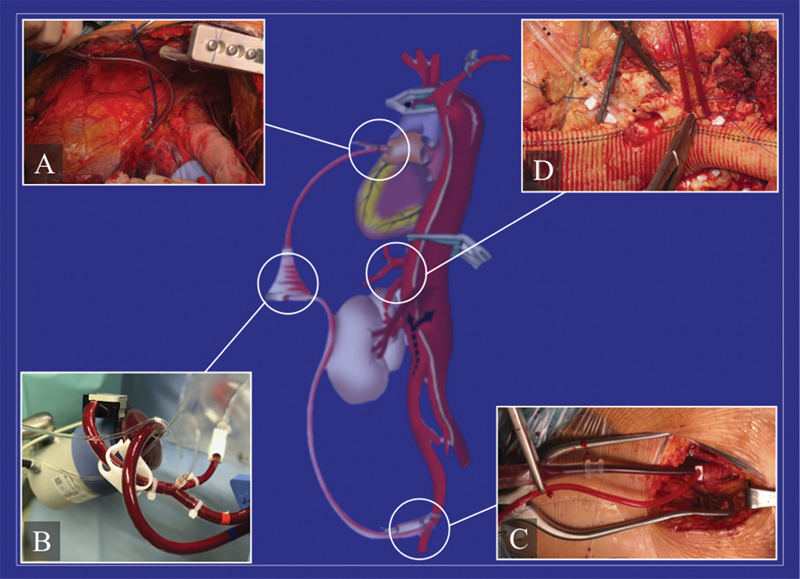
- Coselli J S. The use of left heart bypass in the repair of thoracoabdominal aortic aneurysms: current techniques and results. Semin Thorac Cardiovasc Surg. 2003;15(04):326–332. - PubMed
-
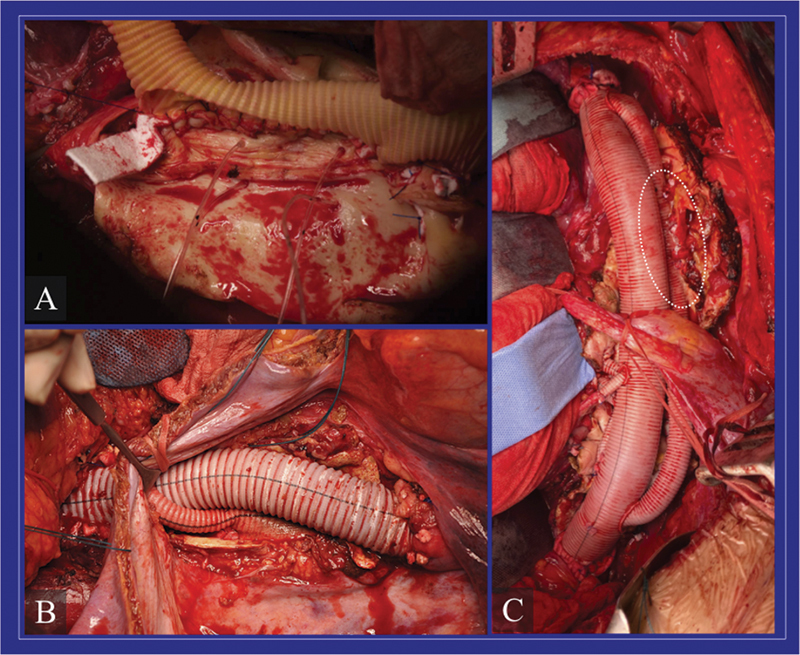
- Ziganshin B A, Elefteriades J A. Surgical management of thoracoabdominal aneurysms. Heart. 2014;100(20):1577–1582. - PubMed
LinkOut - more resources
Full Text Sources