

Incremental medical cost of delirium in elderly patients with cognitive impairment: analysis of a nationwide administrative database in Japan
- PMID: 36521906
- PMCID: PMC9756163
- DOI: 10.1136/bmjopen-2022-062141
Incremental medical cost of delirium in elderly patients with cognitive impairment: analysis of a nationwide administrative database in Japan
Abstract
Objectives: Delirium is a neuropsychiatric disorder that commonly occurs in elderly patients with cognitive impairment. The economic burden of delirium in Japan has not been well characterised. In this study, we assessed incremental medical costs of delirium in hospitalised elderly Japanese patients with cognitive impairment.
Design: Retrospective, cross-sectional, observational study.
Setting: Administrative data collected from acute care hospitals in Japan between April 2012 and September 2020.
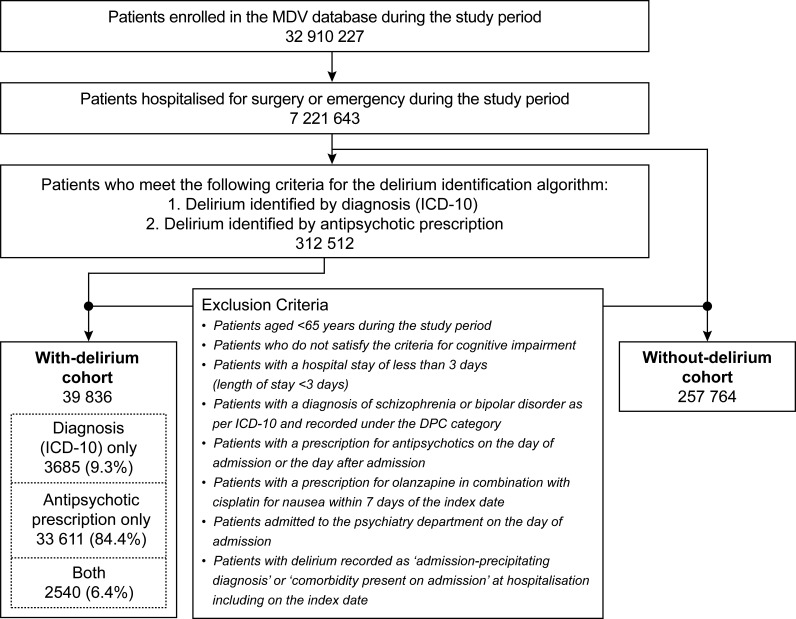
Participants: Hospitalised patients ≥65 years old with cognitive impairment were categorised into groups-with and without delirium. Delirium was identified using a delirium identification algorithm based on the International Classification of Diseases 10th Revision codes or antipsychotic prescriptions.
Outcome measures: Total medical costs during hospitalisation were compared between the groups using a generalised linear model.
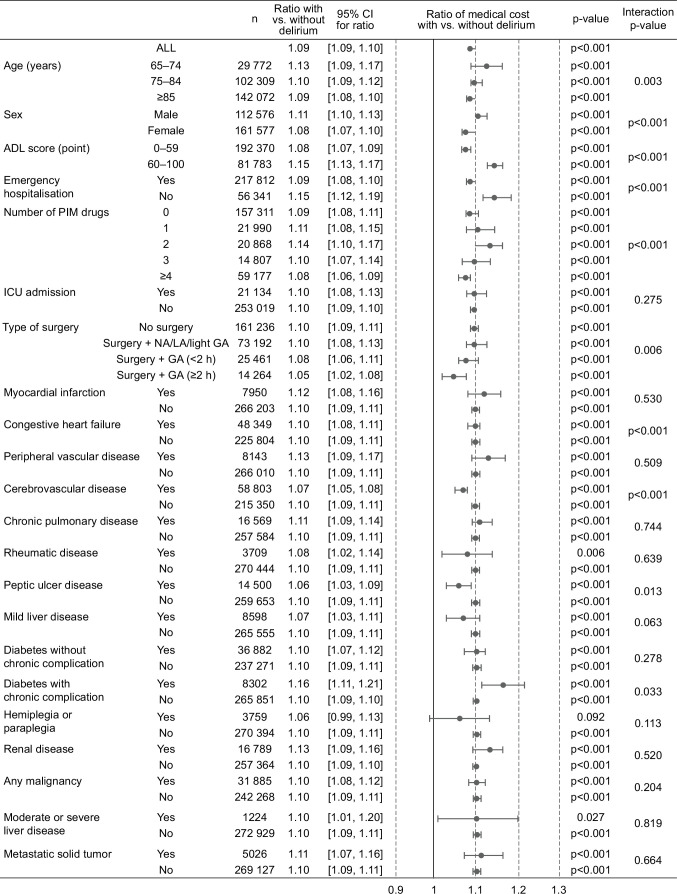
Results: The study identified 297 600 hospitalised patients ≥65 years of age with cognitive impairment: 39 836 had delirium and 257 764 did not. Patient characteristics such as age, sex, inpatient department and comorbidities were similar between groups. Mean (SD) unadjusted total medical cost during hospitalisation was 979 907.7 (871 366.4) yen for patients with delirium and 816 137.0 (794 745.9) yen for patients without delirium. Adjusted total medical cost was significantly greater for patients with delirium compared with those without delirium (cost ratio=1.09, 95% CI: 1.09 to 1.10; p<0.001). Subgroup analyses revealed significantly higher total medical costs for patients with delirium compared with those without delirium in most subgroups except patients with hemiplegia or paraplegia.
Conclusions: Medical costs during hospitalisation were significantly higher for patients with delirium compared with those without delirium in elderly Japanese patients with cognitive impairment, regardless of patient subgroups such as age, sex, intensive care unit admission and most comorbidities. These findings suggest that delirium prevention strategies are critical to reducing the economic burden as well as psychological/physiological burden in cognitively impaired elderly patients in Japan.
Keywords: Delirium & cognitive disorders; Dementia; Old age psychiatry.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MI, KO, NU, HS, KT, ST and SO are employees of MSD KK, Tokyo, Japan, a subsidiary of Merck & Co, Inc, Rahway, New Jersey, USA, and may own stock and/or stock options in Merck & Co, Inc, Rahway, New Jersey, USA. ZPQ was an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co, Inc, Rahway, New Jersey, USA, at the time of the study and may have owned stock and/or stock options in Merck & Co, Inc, Rahway, New Jersey, USA. AO and YO have received funding from MSD KK, Tokyo, Japan, for research consulting.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous