

Assessment of myocardial fibrosis in patients with systemic sclerosis using [68Ga]Ga-FAPI-04-PET-CT
- PMID: 36522438
- PMCID: PMC10119041
- DOI: 10.1007/s00259-022-06081-4
Assessment of myocardial fibrosis in patients with systemic sclerosis using [68Ga]Ga-FAPI-04-PET-CT
Abstract
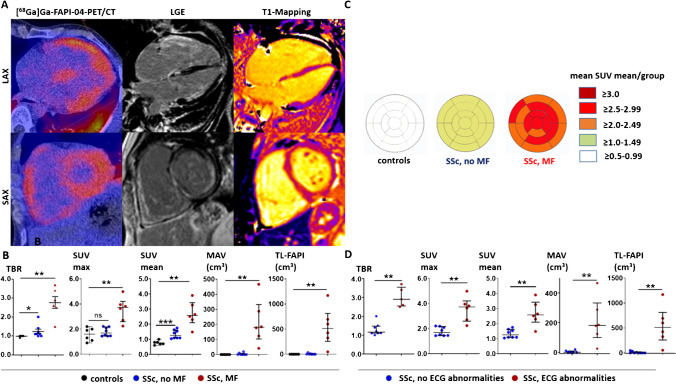
Purpose: Myocardial fibrosis (MF) is a factor of poor prognosis in systemic sclerosis (SSc). Direct in-vivo visualization of fibroblast activation as early readout of MF has not been feasible to date. Here, we characterize 68Gallium-labeled-Fibroblast-Activation-Inhibitor-04 ([68Ga]Ga-FAPI-04)-PET-CT as a diagnostic tool in SSc-related MF.
Methods: In this proof-of-concept trial, six SSc patients with and eight without MF of the EUSTAR cohort Erlangen underwent [68Ga]Ga-FAPI-04-PET-CT and cardiac MRI (cMRI) and clinical and serologic investigations just before baseline and during follow-up between January 2020 and December 2020. Myocardial biopsy was performed as clinically indicated.
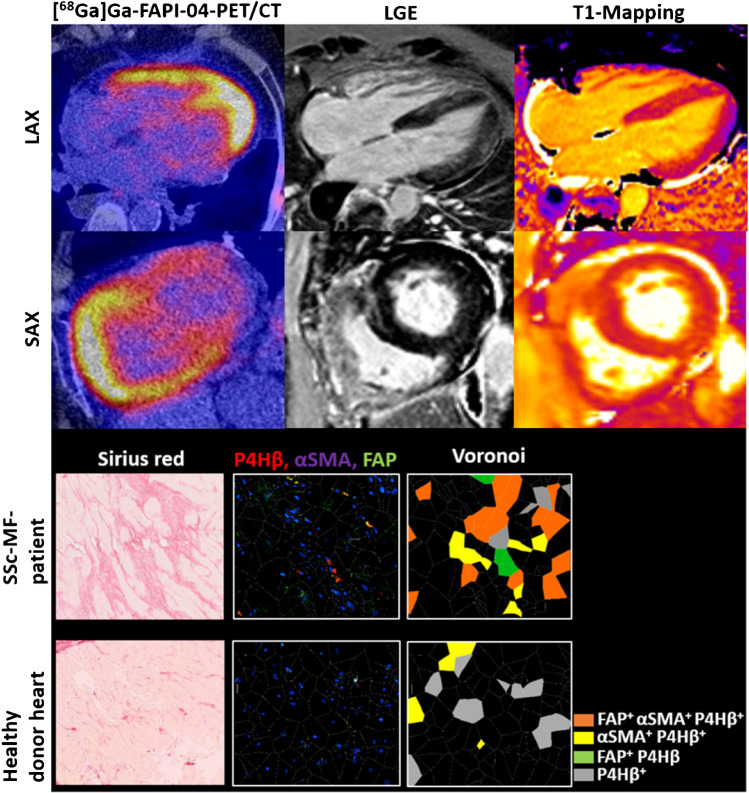
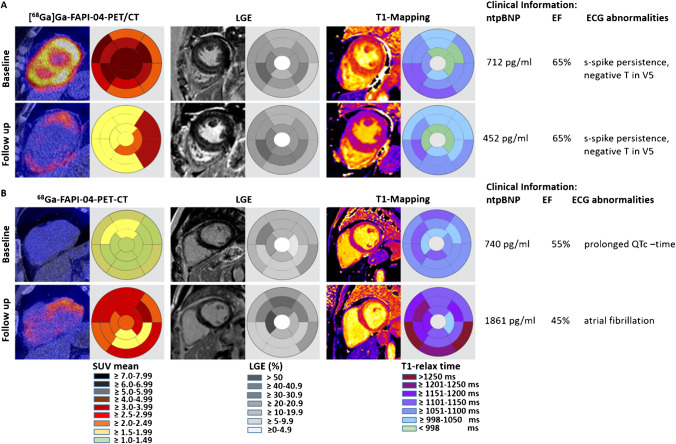
Results: [68Ga]Ga-FAPI-04 tracer uptake was increased in SSc-related MF with higher uptake in SSc patients with arrhythmias, elevated serum-NT-pro-BNP, and increased late gadolinium enhancement (LGE) in cMRI. Histologically, myocardial biopsies from cMRI- and [68Ga]Ga-FAPI-04-positive regions confirmed the accumulation of FAP+ fibroblasts surrounded by collagen deposits. We observed similar but not equal spatial distributions of [68Ga]Ga-FAPI-04 uptake and quantitative cMRI-based techniques. Using sequential [68Ga]Ga-FAPI-04-PET-CTs, we observed dynamic changes of [68Ga]Ga-FAPI-04 uptake associated with changes in the activity of SSc-related MF, while cMRI parameters remained stable after regression of molecular activity and rather indicated tissue damage.
Conclusions: We present first in-human evidence that [68Ga]Ga-FAPI-04 uptake visualizes fibroblast activation in SSc-related MF and may be a diagnostic option to monitor cardiac fibroblast activity in situ.
Keywords: Cardiac MRI; Myocardial fibrosis; Systemic sclerosis; [68Ga]Ga-FAPI-04-PET-CT.
© 2022. The Author(s).
Conflict of interest statement
JHWD has consultancy relationships and/or has received research funding from Actelion, BMS, Celgene, Bayer Pharma, Boehringer Ingelheim, JB Therapeutics, Sanofi-Aventis, Novartis, UCB, GSK, Array Biopharma, Galapagos, Inventiva, and Active Biotech in the area of potential treatments of SSc and is stock owner of 4D Science. CB has received consultancy fees from Pfizer, Janssen, and Boehringer Ingelheim. KT has received consultancy fees and honoraria from UCB and Gilead. CS has received consultancy fees from ROTOP Pharmaka GmbH and Lilly Pharmaceuticals.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
