

Patients with type 1 and type 2 diabetes hospitalized with COVID-19 in comparison with influenza: mortality and cardiorenal complications assessed by nationwide Swedish registry data
- PMID: 36522650
- PMCID: PMC9753889
- DOI: 10.1186/s12933-022-01719-x
Patients with type 1 and type 2 diabetes hospitalized with COVID-19 in comparison with influenza: mortality and cardiorenal complications assessed by nationwide Swedish registry data
Abstract
Background: The risk of severe coronavirus disease 2019 (COVID-19) is increased in people with diabetes, but effects of diabetes type and other risk factors remain incompletely characterized. We studied this in a Swedish cohort of hospitalized patients with type 1 and type 2 diabetes (T1D and T2D), also including comparisons with influenza epidemics of recent years.
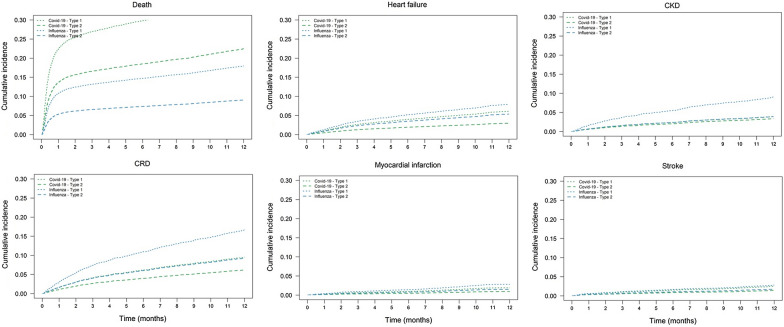
Methods: Nationwide healthcare registries were used to identify patients. A total of 11,005 adult patients with diabetes (T1D, n = 373; T2D, n = 10,632) were hospitalized due to COVID-19 from January 1, 2020 to September 1, 2021. Moreover, 5111 patients with diabetes (304 T1D, 4807 T2D) were hospitalized due to influenza from January 1, 2015 to December 31, 2019. Main outcomes were death within 28 days after admission and new hospitalizations for heart failure (HF), chronic kidney disease (CKD), cardiorenal disease (CRD; composite of HF and CKD), myocardial infarction (MI) and stroke during 1 year of follow-up.
Results: Number of deaths and CRD events were 2025 and 442 with COVID-19 and 259 and 525 with influenza, respectively. Age- and sex-adjusted Cox regression models in COVID-19 showed higher risk of death and HF in T1D vs. T2D, hazard ratio (HR) 1.77 (95% confidence interval 1.41-2.22) and 2.57 (1.31-5.05). With influenza, T1D was associated with higher risk of death compared with T2D, HR 1.80 (1.26-2.57). Older age and previous CRD were associated with higher risks of death and hospitalization for CRD. After adjustment for prior comorbidities, mortality differences were still significant, but there were no significant differences in cardiovascular and renal outcomes. COVID-19 relative to influenza was associated with higher risk of death in both T1D and T2D, HR 2.44 (1.60-3.72) and 2.81 (2.59-3.06), respectively.
Conclusions: In Sweden, patients with T1D as compared to T2D had a higher age- and sex-adjusted risk of death within 28 days and HF within one year after COVID-19 hospitalization, whereas the risks of other non-fatal cardiovascular and renal disease events were similar. Patients with T1D as well as T2D have a greater mortality rate when hospitalized due to COVID-19 compared to influenza, underscoring the importance of vaccination and other preventive measures against COVID-19 for diabetes patients.
Keywords: Cardiovascular complications; Coronavirus 2019 (COVID-19); Mortality; Type 1 diabetes; Type 2 diabetes.
© 2022. The Author(s).
Conflict of interest statement
AstraZeneca was the sponsor of this study. J.B. is a full-time employee of AstraZeneca. J.W.E. has received reimbursement for consultancies or research support from Novo Nordisk, Merck Sharp & Dohme, Boehringer Ingelheim, Ilya Pharma and AstraZeneca. A.N. has received honoraria from MSD, AstraZeneca, Eli Lilly, Boehringer Ingelheim, and Novo Nordisk. M.T. is employed by an independent statistical consultant company, Statisticon AB, of which AstraZeneca Nordic-Baltic is a client. D.N. has received consultancy fees from Novo Nordisk, AstraZeneca, and Eli Lilly. T.N. has received unrestricted grants from AstraZeneca and Novo Nordisk and has served on national advisory boards of Novo Nordisk, Sanofi-Aventis, Eli Lilly, MSD and Boehringer Ingelheim. V.R. has received honoraria from AstraZeneca, Novo Nordisk, and Boehringer Ingelheim on expert group participation. No other potential conflicts of interest relevant to this article were reported.
Figures
References
-
- WHO/Europe | Coronavirus disease (COVID-19) outbreak - WHO announces COVID-19 outbreak a pandemic [Internet]. https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus.... Accessed 16 Jun 2021.
-
- WHO Coronavirus (COVID-19) Dashboard | WHO coronavirus (COVID-19) dashboard with vaccination data [Internet]. https://covid19.who.int/. Accessed 14 Sep 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
