

doi: 10.1002/joa3.12714.
eCollection 2022 Dec.
JCS/JHRS 2020 Guideline on Pharmacotherapy of Cardiac Arrhythmias
- PMID: 36524037
- PMCID: PMC9745564
- DOI: 10.1002/joa3.12714
Item in Clipboard
JCS/JHRS 2020 Guideline on Pharmacotherapy of Cardiac Arrhythmias
J Arrhythm.
.
No abstract available
Figures
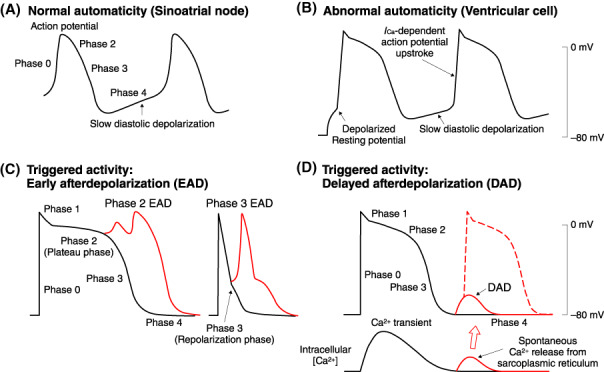
Normal (A) and abnormal (B) automaticity, and triggered activities mediated by either early afterdepolarization (C) or delayed afterdepolarization (D).
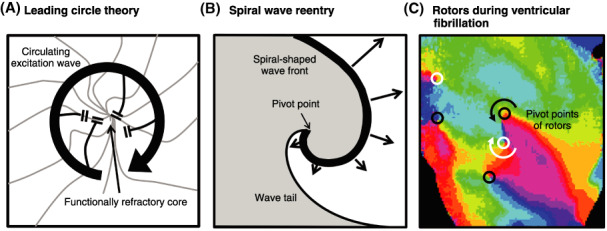
(A) Leading circle theory (Source: Prepared base on Allessie MA et al. 1977
9
). (B) Spiral wave reentry (Source: Prepared base on Pertsov AM et al. 1993
10
). (C) Multiple rotors during ventricular fibrillation. Pivot points can be identified by convergence of all phases of the action potential (Source: Prepared base on Harada M et al. 2008
11
).
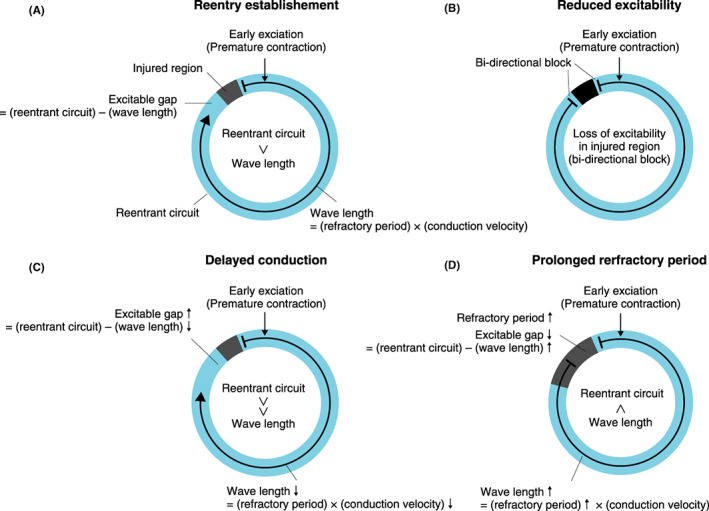
Scheme for reentrant arrhythmia and effects of antiarrhythmic drugs. The situation where early exciation (premature contraction) (vertical arrow) penetrates in the reentrant circuit (blue circle) in vicinity of damaged tissue (gray or black box). (A) Without anti‐arrhyhmic drugs. (B) Drugs that reduce excitability, such as class I drugs. (C) Drugs that delay conduction, such as class IC drugs. (D) Drugs that prolong refractory period, such as class III drugs.
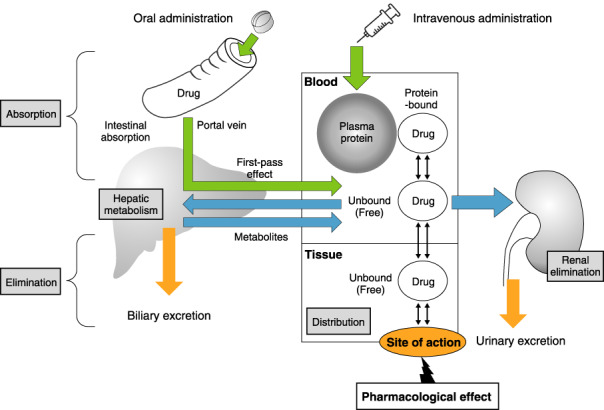
Pharmacokinetics (absorption, distribution, metabolism, and elimination).
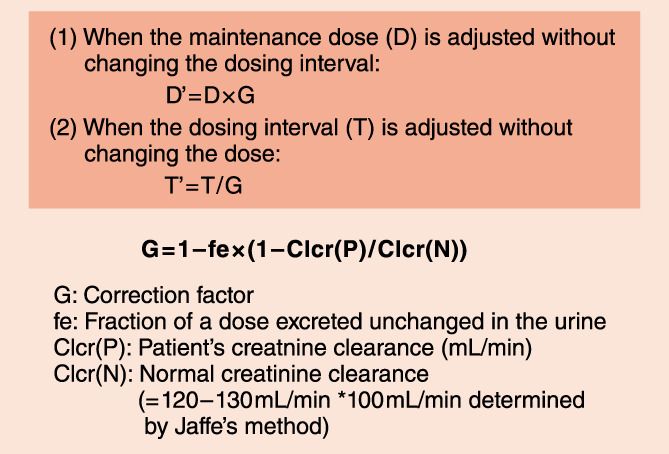
Dose adjustment for patients with renal dysfunction: the Giusti‐Hayton method.
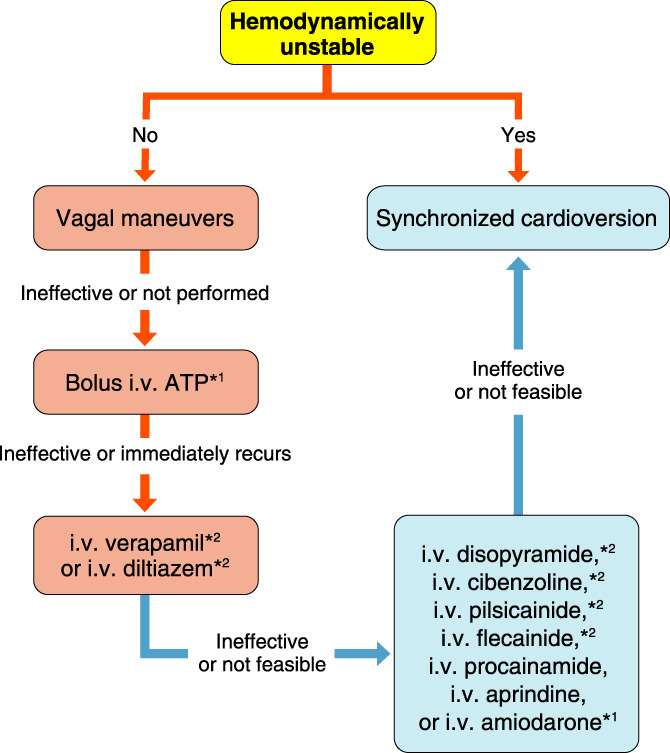
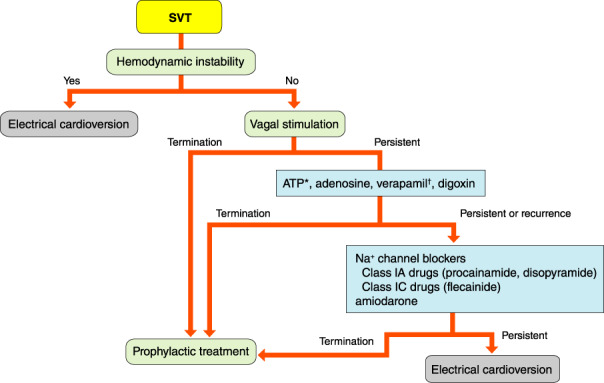
Acute treatment of narrow QRS supraventricular tachycardia. *1Off‐label use in Japan. *2Contralndicated in pts with reduced systolic function. ATP, adenosine triphosphate
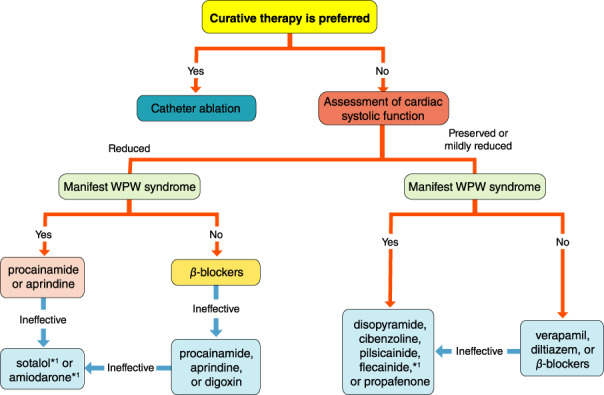
Prophylactic therapy of supraventricular tachycardia. *1Off‐label use in Japan. WPW, Wolff‐Parkinson‐White.
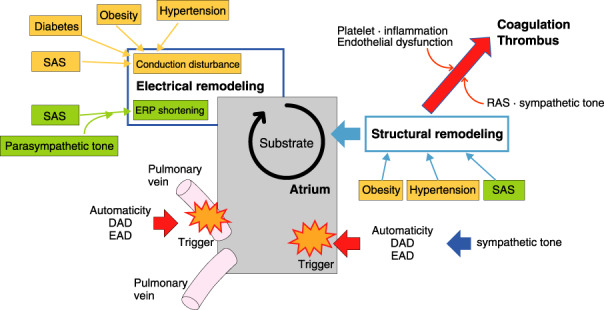
Risk factors contributing to both atrial remodeling and formation of thrombus. DAD, delayed afterdepolarization; EAD, early afterdepolarization; ERP, effective refractory period; RAS, renin–angiotensin system; SAS, sleep apnea syndrome.
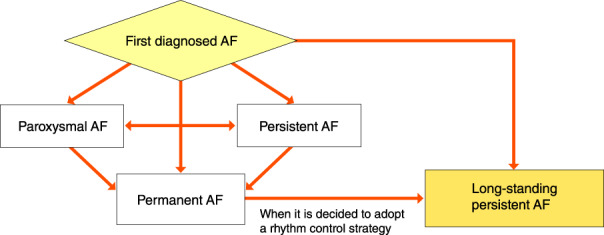
Classification of AF. AF, atrial fibrillation. (Source: Prepared based on Fuster V, et al. 2011, Fuster V, et al. 2006.
203
).
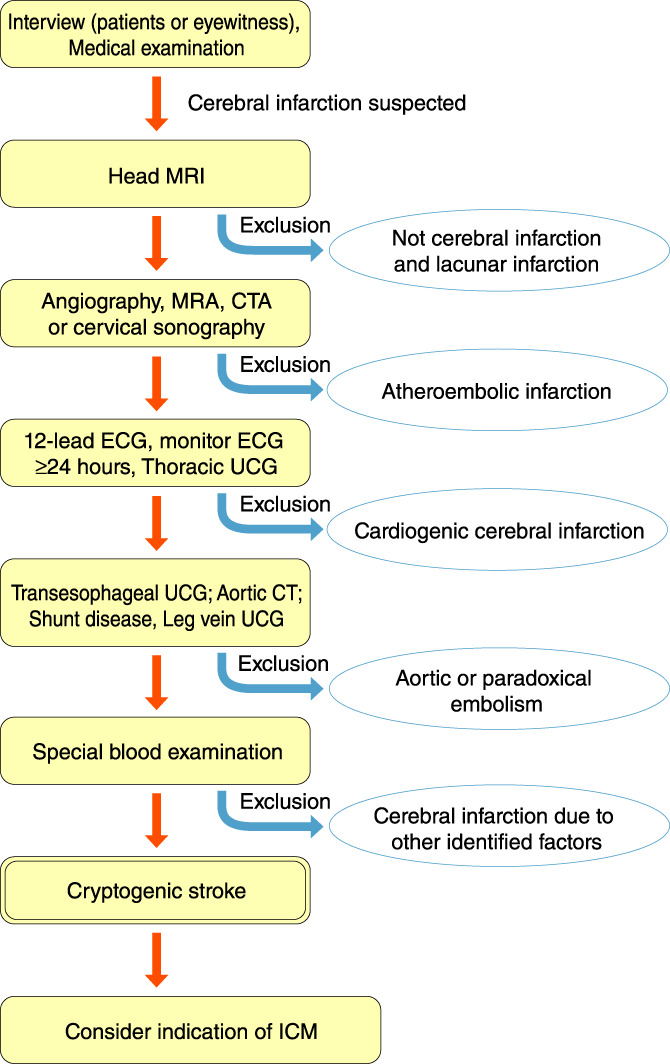
Flow chart for indication of ICM in patients with cryptogenic stroke. CT, computed tomography; CTA, computed tomography angiography; ECG, electrocardiogram; ICM, insertable cardiac monitor; MRA, mineralocorticoid‐receptor antagonist; MRI, magnetic resonance imaging; UCG, ultrasonic echocardiography. (Adapted from the Japan Stroke Society. 2016.
218
)
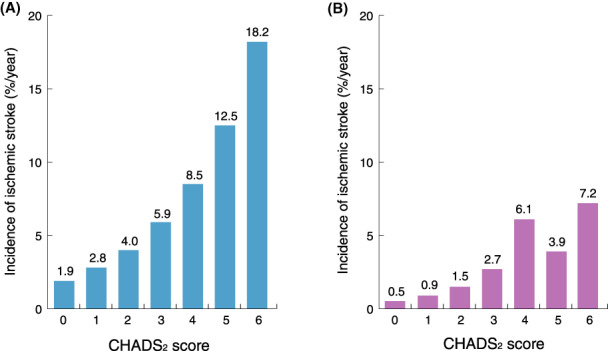
Incidence rates of ischemic stroke for each CHADS2 score. (A) Incidence rates of ischemic stroke with the original CHADS2 score (Adapted from Gage BF et al, 2001
245
). (B) Incidence rates of ischemic stroke in Japanese patients not receiving anticoagulation therapy (pooled analysis of the J‐RHYTHM Registry, Fushimi AF Registry, and Shinken Database). (Adapted from Suzuki S et al, 2015
252
)
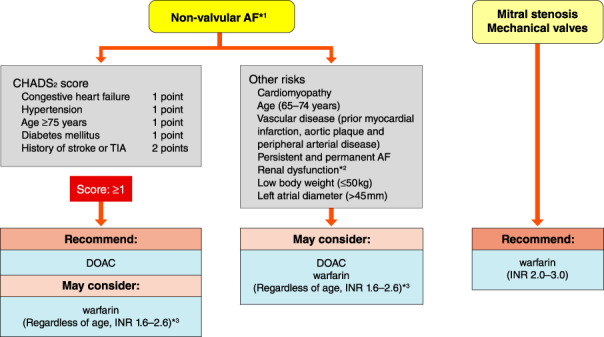
Anticoagulation therapy in AF. *Bioprosthetic values are included in non‐valvular AF. *2Regarding anticoagulation according to renal function, see “3.2.3 Selection of Direct Oral Anticoagulants” and Table 36. *3Regarding target INR 1.6–2.6 in non‐valvular AF, INR close to 2.0 is recommended as possible. INR 2.0–3.0 may be considered in high‐risk patients aged <70 years with a history of stroke or CHADS2 score ≥3. AF, atrial fibrillation; DOAC, direct oral anticoagulant; INR, international normalized ratio; TIA, transient ischemic attack.
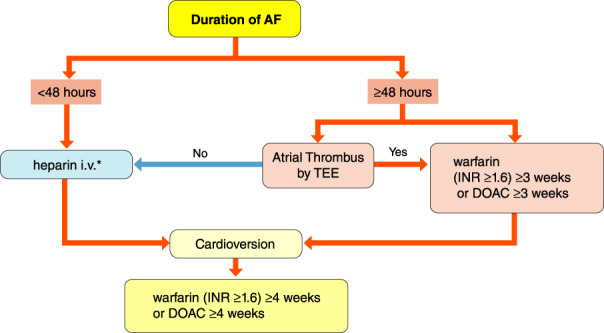
Anticoagulant therapy for cardioversion. *2,000–5,000 U unfractionated heparin i.v. (evidence for the dose is poor). In case of AF lasting <48 h without anticoagulants, DOAC is recommended unless contraindicated as the effect of anticoagulation is rapid. AF, atrial fibrillation; DOAC, direct oral anticoagulant; INR, international normalized ratio; TEE, transesophageal echocardiography.
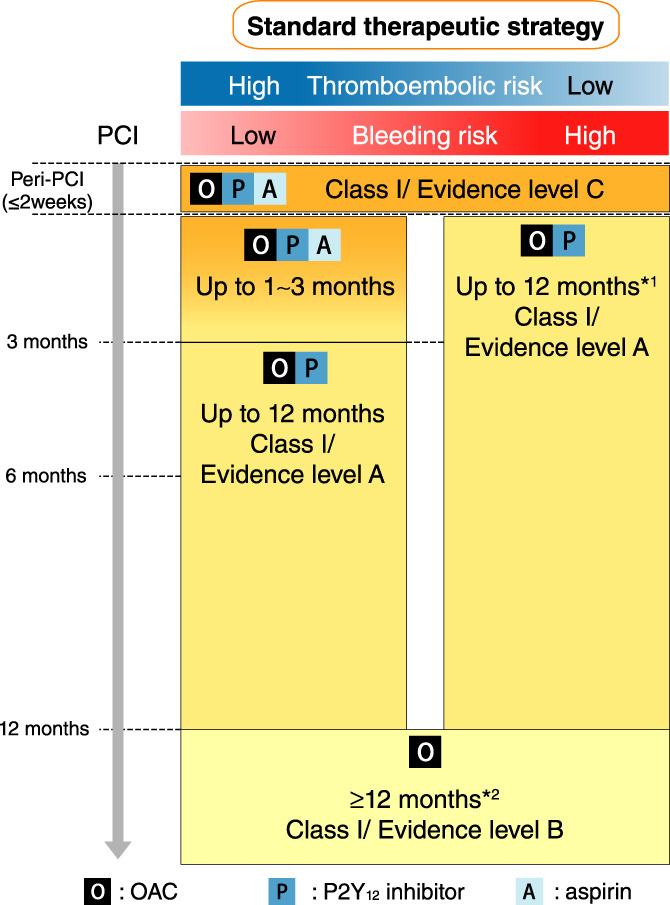
Recommended choice and duration of antithrombic therapy in atrial fibrillation concomitant with ischemic heart disease. *1Short duration of 6 months of dual therapy can be considered in patients with a very high bleeding risk. *2Continuation of dual therapy with an OAC and aspirin (or P2Y12 inhibitor) for longer than 12 months can be considered in patients with a very high thromboembolic risk. PCI, percutaneous coronary intervention, OAC, oral anticoagulant.
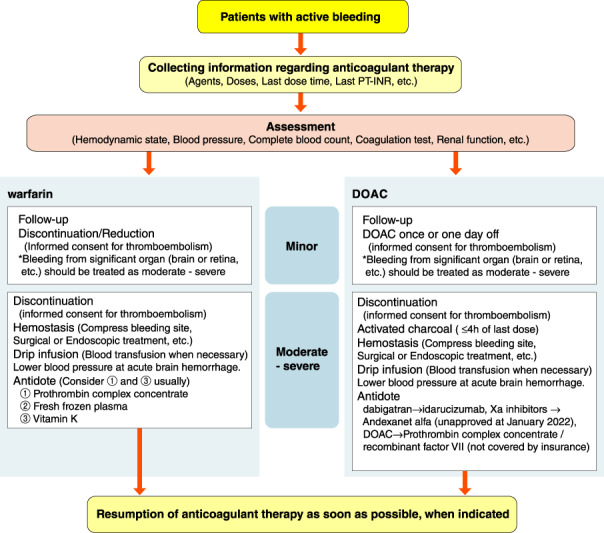
Treatment for active bleeding during anticoagulant therapy in patients with atrial fibrillation. DOAC, direct oral anticoagulant; PT‐INR, prothrombin time‐international normalized ratio.
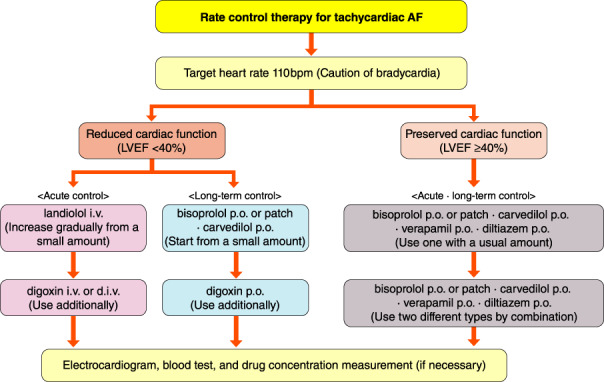
Treatment flowchart of rate control therapy for tachycardiac AF. AF, atrial fibrillation; LVEF, left ventricular ejection fraction.
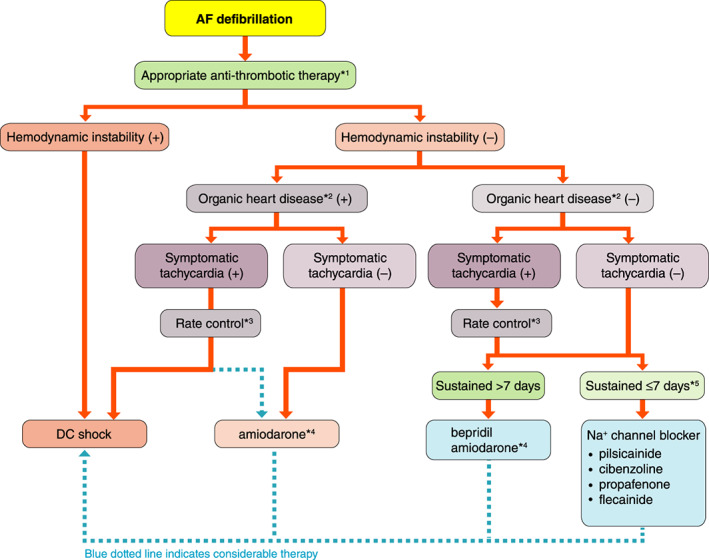
Flow‐chart for defibrillation of AF. *1The possibility of 48‐h continuation of AF cannot be denied; essential to confirm the absence of intra‐atrial thrombus by transesophageal echocardiography or to perform appropriate anticoagulation therapy for 3 weeks (see “Chapter V. 3. Anticoagulation Therapy” for details). *2Hypertrophic heart, heart failure, ischemic heart disease. *3Even without hemodynamic instability, rate control therapy might be combined in cases of symptomatic tachycardia (see “Chapter V. 4. Rate Control Therapy” for details). *4Insurance coverage for Amiodarone is approved only for patients with AF with hypertrophic cardiomyopathy or heart failure in Japan. *5Rhythm control therapy should be performed within 48 h of AF onset by considering efficacy of therapy as well as prevention of systemic embolism. AF, atrial fibrillation; DC, direct‐current.
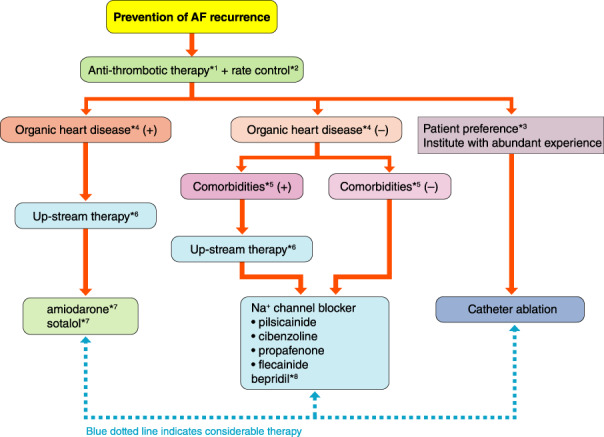
Flowchart for prevention of AF. *1Anticoagulation therapy might be continued depending on individual risks for embolism and efficacy of AF preventive therapy (see “Chapter V. 3 Anticoagulation Therapy” for details). *2Rate control therapy might be continued in cases of possible AF recurrence and considerable symptoms during AF (see “Chapter V. 4 Rate Control Therapy” for details). *3See the “Guidelines for Non‐Pharmacological Therapy”, 2018 edition 3 for details. *4Hypertrophic heart, heart failure, ischemic heart disease. *5Hypertension, dyslipidemia, diabetes, obesity, chronic kidney disease, sleep apnea syndrome, etc. (see “Chapter V. 2.5 Management of Risk Factors and Comorbidity” for details). *6Appropriate therapeutic intervention for basic and/or complicated diseases (see “Chapter V. 6 Upstream Therapy” for details). *7Insurance coverage for amiodarone is approved in Japan only for patients with AF and hypertrophic cardiomyopathy or heart failure. Insurance coverage for sotalol is not approved for patients with AF, although the efficacy of sotalol on AF complicated with ischemic heart disease. *8bepridil is reported to be effective for AF with ventricular dysfunction; however there are reports warning of exaggeration of proarrhythmia. AF, atrial fibrillation.
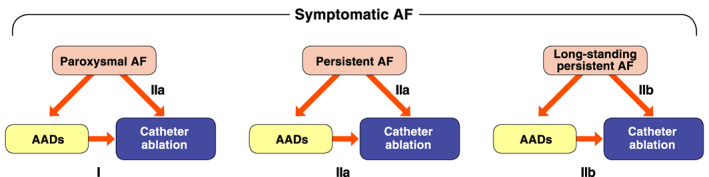
Flowchart diagram of treatment for symptomatic AF patients based on its persistence. AAD, anti‐arrhythmic drugs; AF, atrial fibrillation; CA, catheter ablation. (Adapted from the Japanese Circulation Society 2019
3
)
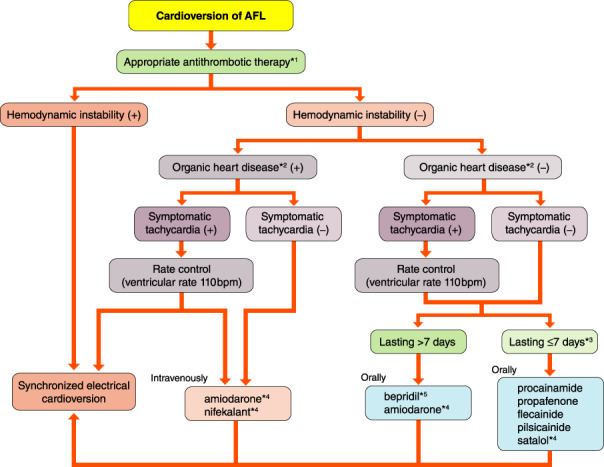
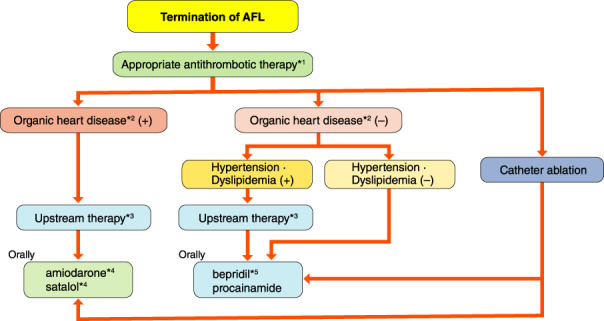
Pharmacotherapy to restore sinus nodal rhythm in patient with hemodynamically stable AFL. *1Adequate anticoagulant therapy is required in patients with AFL for 3 weeks before cardioversion and 4 weeks after if it is unclear whether AFL lasts for ≤48 h. *2Cardiac hypertrophy, cardiac dysfunction and cardiac ischemia. *3In order to ensure efficacy and prevent thromboembolic complications, the duration of an AFL episode should be limited to ≤48 h. *4Class III antiarrhythmic drugs are not covered by the National Health Insurance in Japan. *5bepridil is not indicated for AFL in Japan. AFL, atrial flutter.
Pharmacotherapy to prevent AFL recurrence. *1Continuous rate control therapy is recommended for patients in whom it is not impossible for there to be recurrence of symptomatic AFL regardless of pharmacotherapy. *2Cardiac hypertrophy, cardiac dysfunction and cardiac ischemia. *3Appropriate therapeutic intervention to patient’s underlying disease. *4amiodarone is not indicatd for AFL in Japan. *5bepridil is not indicatd for AFL in Japan. AFL, atrial flutter.
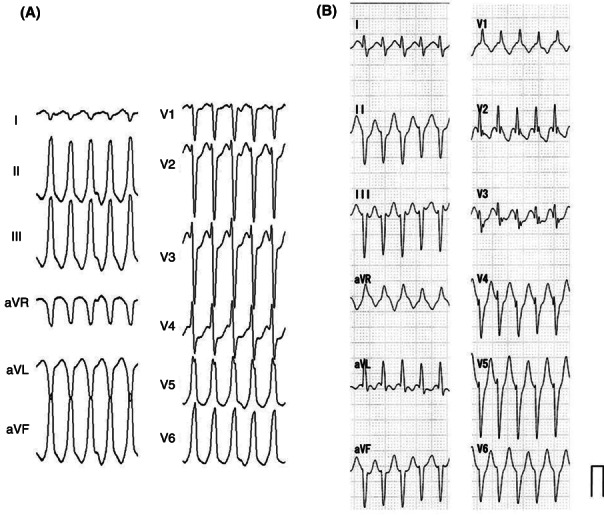
The 12‐lead ECGs during typical idiopathic VT. (A) Idiopathic VT with left bundle branch block and right axis deviation, (B) Idiopathic VT with right bundle branch block and left axis deviation. ECG, electrocardiogram; VT, ventricular tachycardia.
Choice of antiarrhythmic drugs based on the ECG morphology of VT. Intravenous (i.v.) drugs should be injected gradually, and oral (p.o.) drugs should be started with a lower dose. *No insurance reimbursement in Japan. ECG, electrocardiogram. LAD, left axis deviation; LBBB, left bundle branch block; RAD, right axis deviation; RBBB, right bundle branch block; VT, ventricular tachycardia.
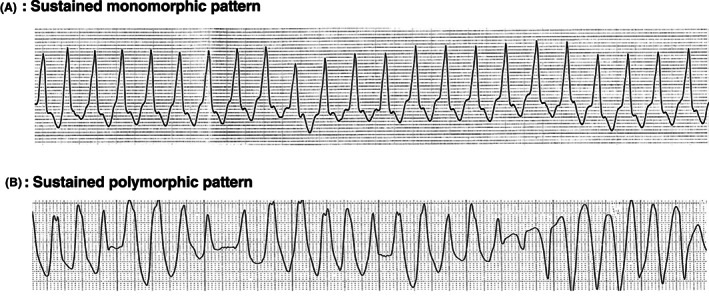
Monitoring ECGs of sustained ventricular tachycardia associated with organic heart disease. ECG, electrocardiogram. (Adapted from Ikeda T 2011.
738
)
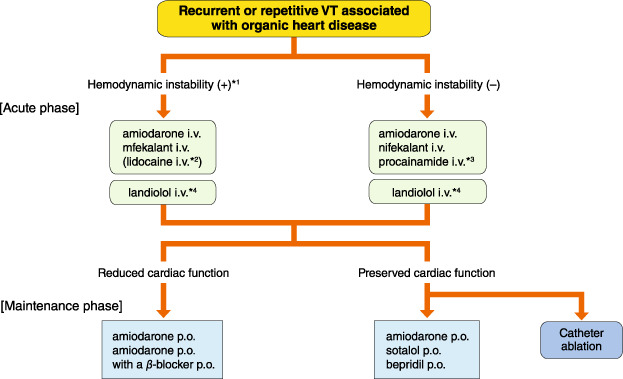
Drug selection for the purpose of termination and prevention of sustained VT associated with organic heart disease. *1In the cases of sustaining hemodynamically unstable tachycardia, the drug should be administered where immediate direct current defibrillation can be performed. *2Alternative drug when no other antiarrhythmic drug is available. *3The drug should be used only for the monomorphic sustained VT. *4The drug should be initiate from low dose and gradually increase for sustained VT. VT, ventricular tachycardia.

Ambulatory ECG Monitoring at the time of initiation of short‐coupled TdP. ECG, electrocardiogram; TdP, torsade de pointes.
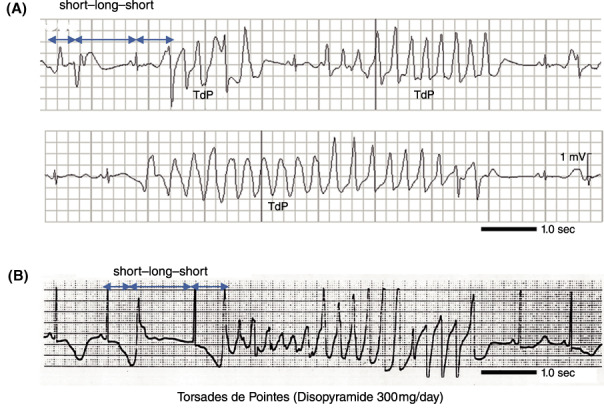
(A) Monitoring ECGs of polymorphic ventricular tachycardia (Torsade de Pointes) with syncope in a patient with LQT2. Change in the R‐R interval (short–long–short) followed by polymorphic ventricular tachycardia, TdP, characterized as a twisting QRS axis. (B) Secondary (Drug) induced QT prolongation. Drug‐induced TdP due to oral disopyramide (300 mg/day). A similar short–long–short change in R‐R followed by TdP. ECG, electrocardiogram; LQT2, long QT syndrome type 2; TdP, torsade de pointes.
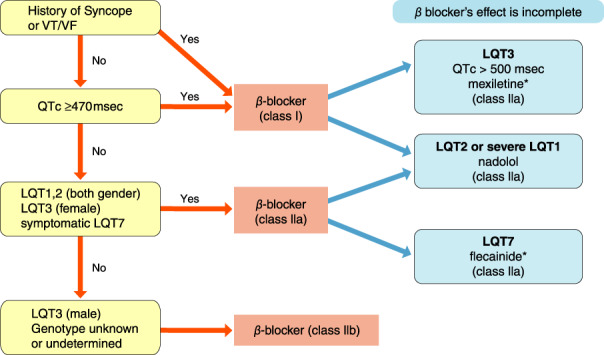
Chronic pharmacological treatment for prevention of TdP in congenital LQTS. *Add to β‐blockers. LQTS, long QT syndrome; TdP, torsade de pointes; VF, ventricular fibrillation; VT, ventricular tachycardia.
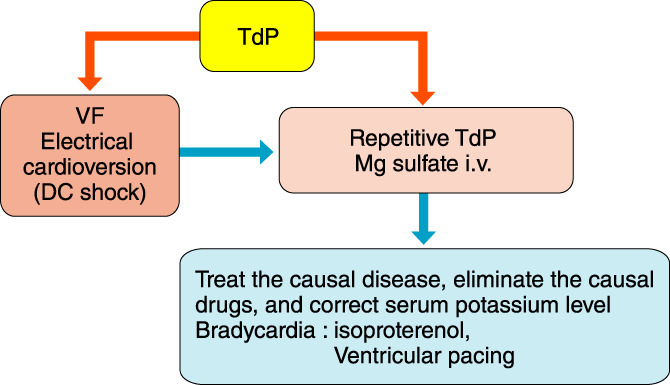
Acute pharmacological treatment for TdP in congenital or acquired LQTS. DC, direct current; LQTS, long QT syndrome; TdP, torsade de pointes; VF, ventricular fibrillation.
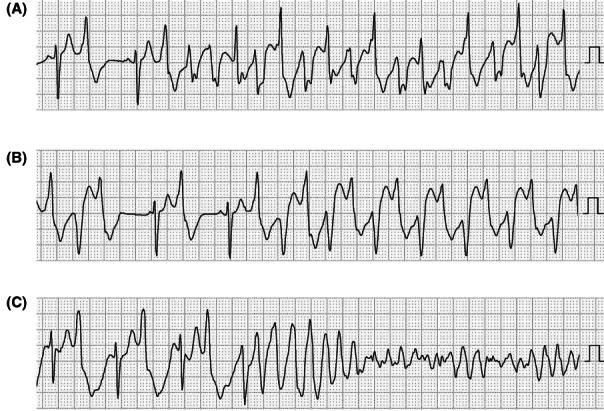
Monitoring ECGs at VT in patients with CPVT: (A) polymorphic VT, (B) bidirectional VT, (C) polymorphic VT leading to ventricular fibrillation. CPVT, catecholaminergic polymorphic ventricular tachycardia; ECG, electrocardiogram; VT, ventricular tachycardia. (Adapted from Sumitomo N et al. 2016.
823
)
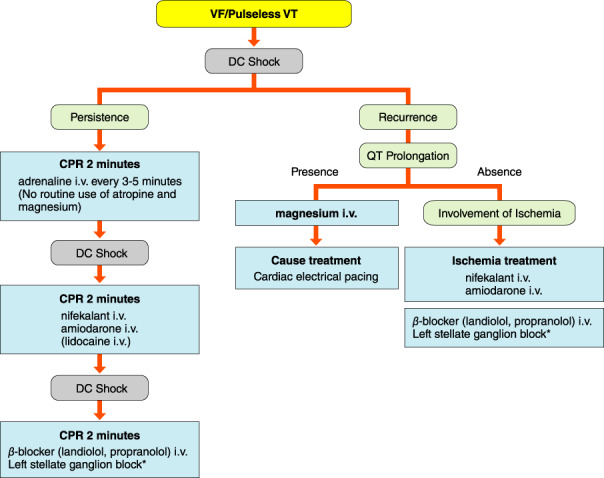
Treatment flowchart for VF/pulseless VT. *Please refer to Figure 32. CPR, cardiopulmonary resuscitation; DC, direct‐current; VF, ventricular fibrillation; VT, ventricular tachycardia.
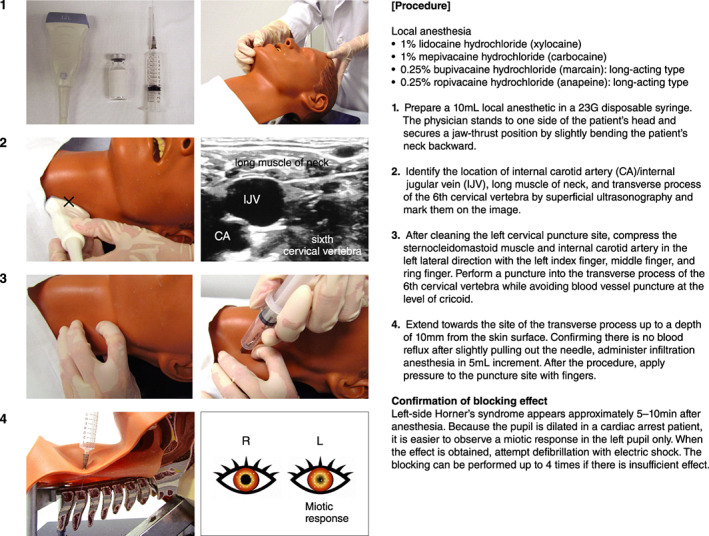
Procedure of left stellate ganglion block for refractory VT/VF. CA, carotid artery; IJV, internal jugular vein; VF, ventricular fibrillation; VT, ventricular tachycardia.
Flow chart to terminate SVT in children. *Off‐label. †Contraindicated for neonates and infants. ATP, adenosine triphosphate; SVT, supraventricular tachycardia.
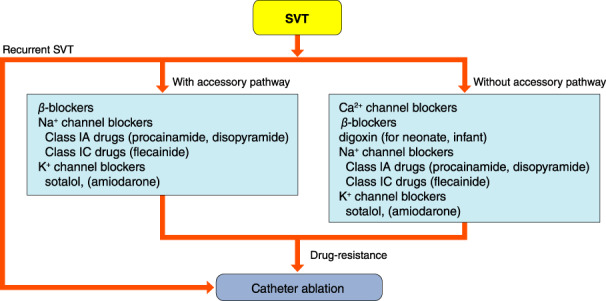
Prophylactic treatment of SVT in children. SVT, supraventricular tachycardia.
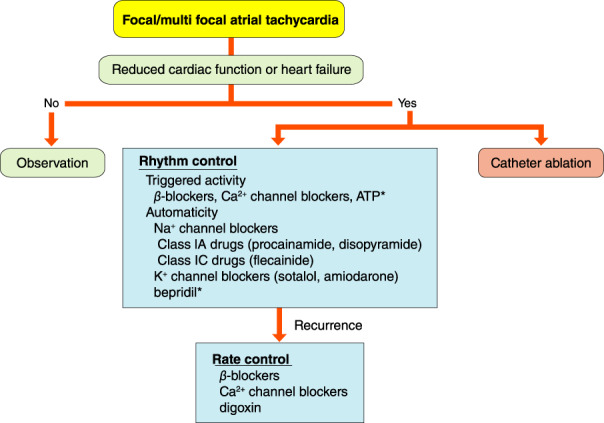
Treatment of atrial tachycardia. *Off‐label. ATP, adenosine triphosphate.
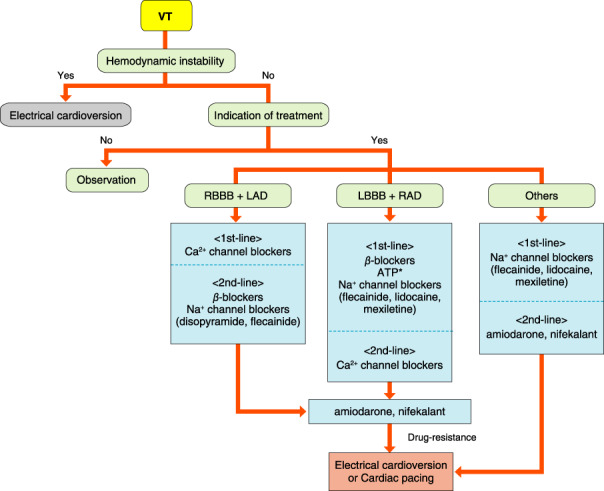
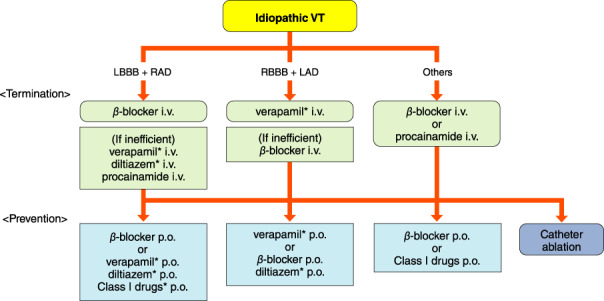
Termination of VT. *Off‐label. ATP, adenosine triphosphate; LAD, left axis deviation; LBBB, left bundle branch block; RAD, right axis deviation; RBBB, right bundle branch block; VT, ventricular tachycardia.
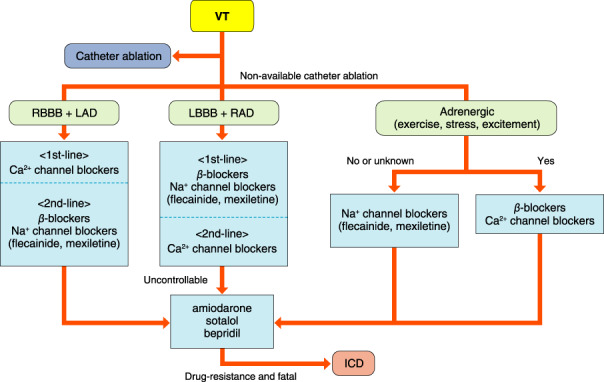
Prophylactic treatment of VT. ICD, implantable cardioverter‐defibrillator; LAD, left axis deviation; LBBB, left bundle branch block; RAD, right axis deviation; RBBB, right bundle branch block; VT, ventricular tachycardia.
References
-
- Japanese Circulation Society Joint Working Group . Guidelines for Drug Treatment of Arrhythmias (JCS) 2009. [in Japanese] Available at: https://www.j‐circ.or.jp/cms/wp‐content/uploads/2020/02/JCS2009_kodama_h... (accessed October 6, 2021).
-
- Japanese Circulation Society Joint Working Group . Guidelines for Pharmacotherapy of Atrial Fibrillation (JCS 2013). Circ J. 2014;78:1997–2021. - PubMed
-
- Mind Treatment Guideline Selection Committee . Fukui T, Yoshida M, Yamaguchi N, editors. Minds handbook for clinical practice guideline development. [in Japanese] Igaku‐Shoin, 2007.
-
- Japanese Circulation Society and Japanese Heart Rhythm Society Joint Working Group . JCS/JHRS 2019 guideline on non‐pharmacotherapy of cardiac arrhythmias. Circ J. 2021;85:1104–244. - PubMed
-
- Japanese Circulation Society Joint Working Group . Guidelines for Diagnosis and Management of Inherited Arrhythmias (JCS) 2017. [in Japanese] Available at: https://www.j‐circ.or.jp/cms/wp‐content/uploads/2020/02/JCS2017_aonuma_h... (accessed October 6, 2021).
LinkOut - more resources
Full Text Sources
