

Empagliflozin protects mice against diet-induced obesity, insulin resistance and hepatic steatosis
- PMID: 36525084
- PMCID: PMC9947060
- DOI: 10.1007/s00125-022-05851-x
Empagliflozin protects mice against diet-induced obesity, insulin resistance and hepatic steatosis
Abstract
Aims/hypothesis: Sodium-glucose cotransporter 2 (SGLT2) inhibitors are widely used in the treatment of type 2 diabetes, heart failure and chronic kidney disease. Their role in the prevention of diet-induced metabolic deteriorations, such as obesity, insulin resistance and fatty liver disease, has not been defined yet. In this study we set out to test whether empagliflozin prevents weight gain and metabolic dysfunction in a mouse model of diet-induced obesity and insulin resistance.
Methods: C57Bl/6 mice were fed a western-type diet supplemented with empagliflozin (WDE) or without empagliflozin (WD) for 10 weeks. A standard control diet (CD) without or with empagliflozin (CDE) was used to control for diet-specific effects. Metabolic phenotyping included assessment of body weight, food and water intake, body composition, hepatic energy metabolism, skeletal muscle mitochondria and measurement of insulin sensitivity using hyperinsulinaemic-euglycaemic clamps.
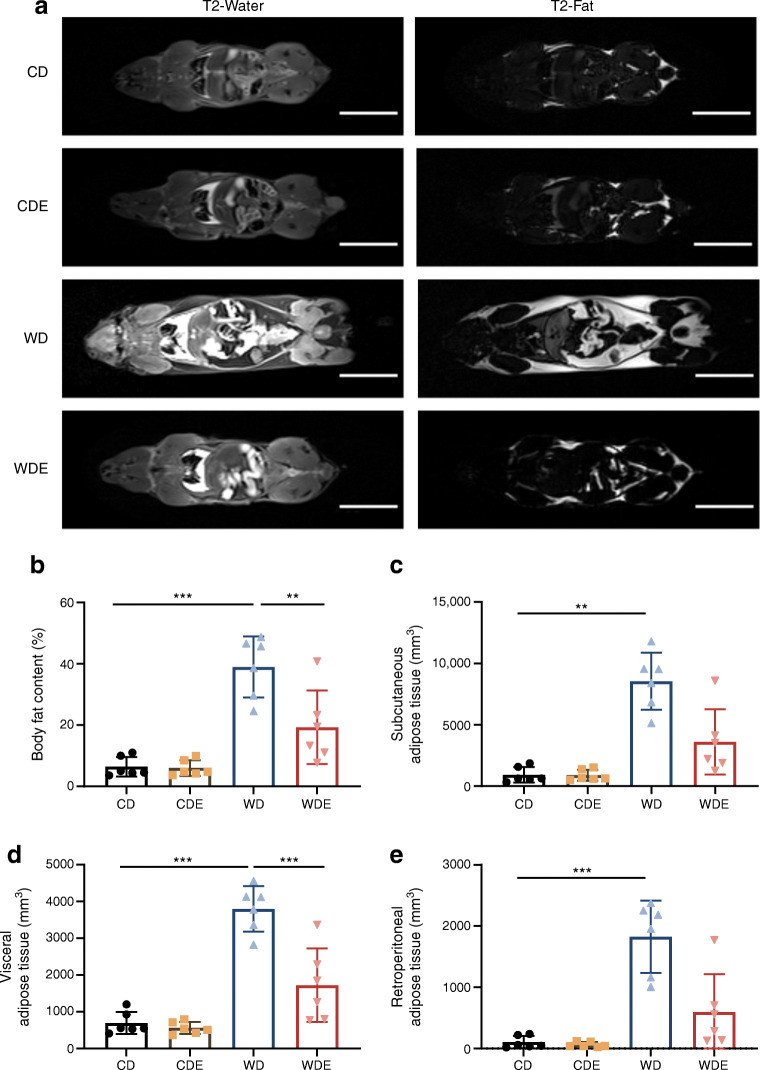
Results: Mice fed the WD were overweight, hyperglycaemic, hyperinsulinaemic and insulin resistant after 10 weeks. Supplementation of the WD with empagliflozin prevented these metabolic alterations. While water intake was significantly increased by empagliflozin supplementation, food intake was similar in WDE- and WD-fed mice. Adipose tissue depots measured by MRI were significantly smaller in WDE-fed mice than in WD-fed mice. Additionally, empagliflozin supplementation prevented significant steatosis found in WD-fed mice. Accordingly, hepatic insulin signalling was deteriorated in WD-fed mice but not in WDE-fed mice. Empagliflozin supplementation positively affected size and morphology of mitochondria in skeletal muscle in both CD- and WD-fed mice.
Conclusions/interpretation: Empagliflozin protects mice from diet-induced weight gain, insulin resistance and hepatic steatosis in a preventative setting and improves muscle mitochondrial morphology independent of the type of diet.
Keywords: Empagliflozin; Insulin resistance; Obesity; SGLT2 inhibition; Skeletal muscle mitochondria; Steatosis; Western-type diet.
© 2022. The Author(s).
Figures





References
-
- World Health Organization (2021) Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 5 Oct 2021
-
- Lingvay I, Sumithran P, Cohen RV, le Roux CW (2021) Obesity management as a primary treatment goal for type 2 diabetes: time to reframe the conversation. Lancet S0140-6736(21)01919-X. 10.1016/S0140-6736(21)01919-X - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
