

Identification and prediction of Parkinson's disease subtypes and progression using machine learning in two cohorts
- PMID: 36526647
- PMCID: PMC9758217
- DOI: 10.1038/s41531-022-00439-z
Identification and prediction of Parkinson's disease subtypes and progression using machine learning in two cohorts
Abstract
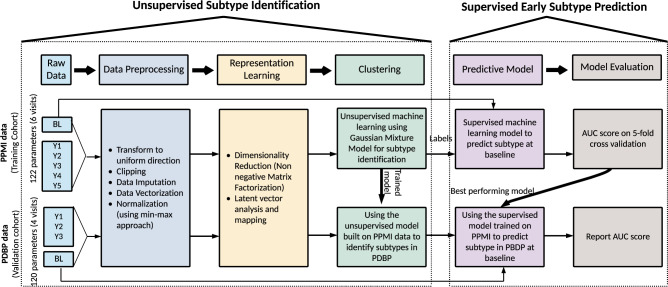
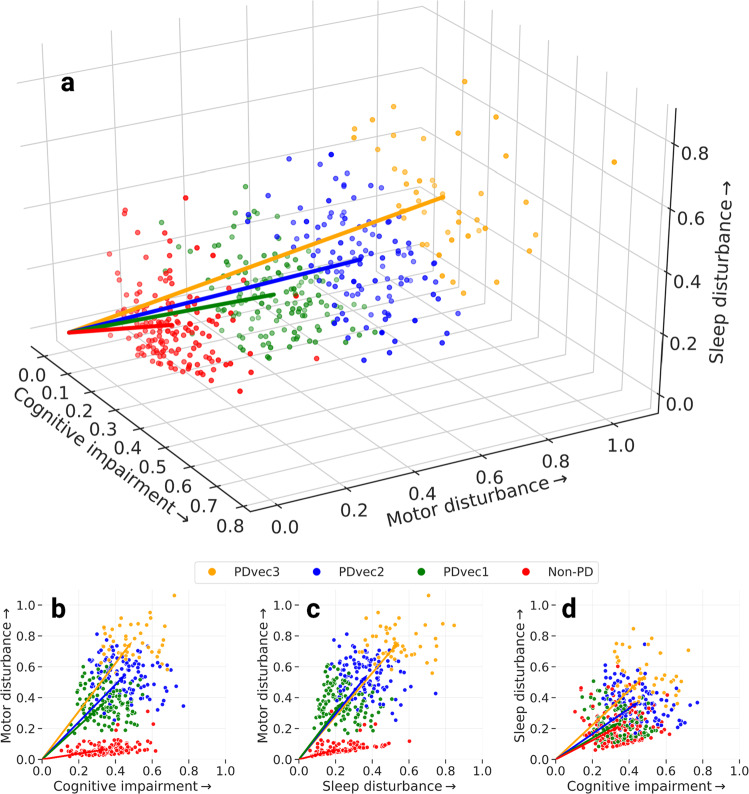
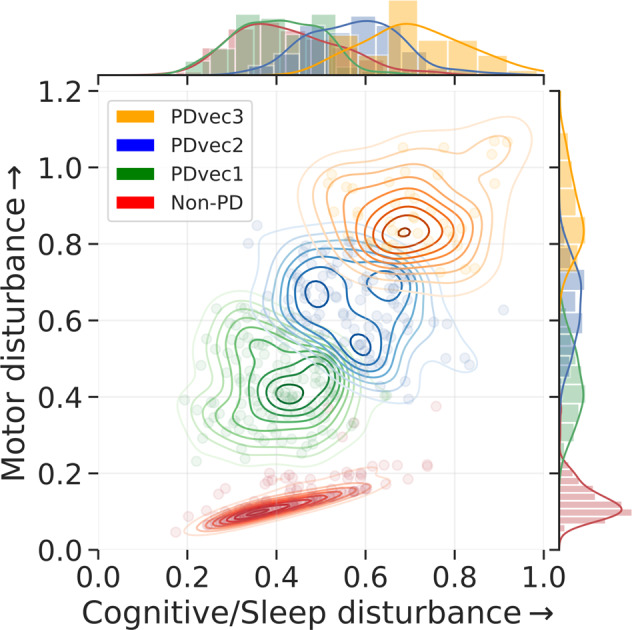
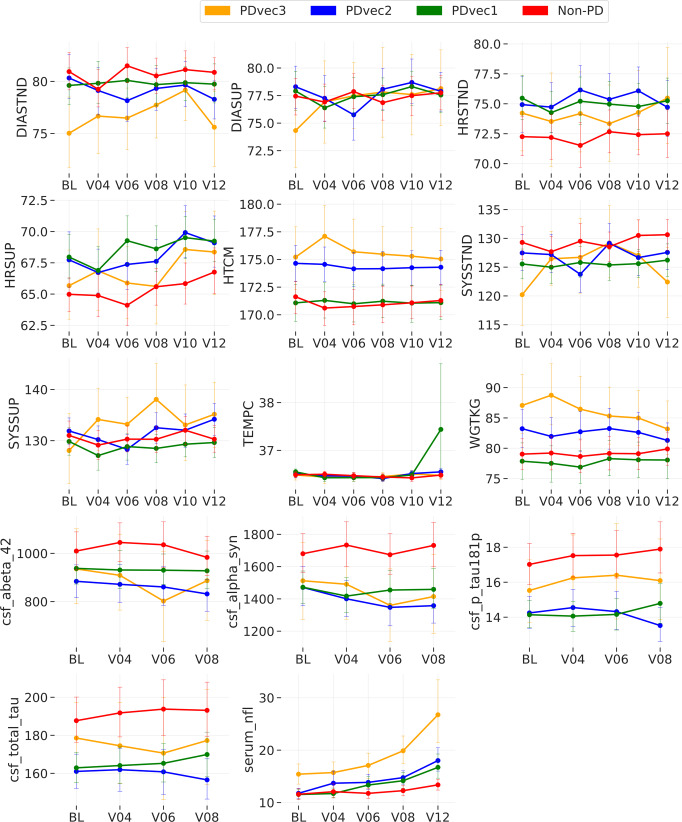
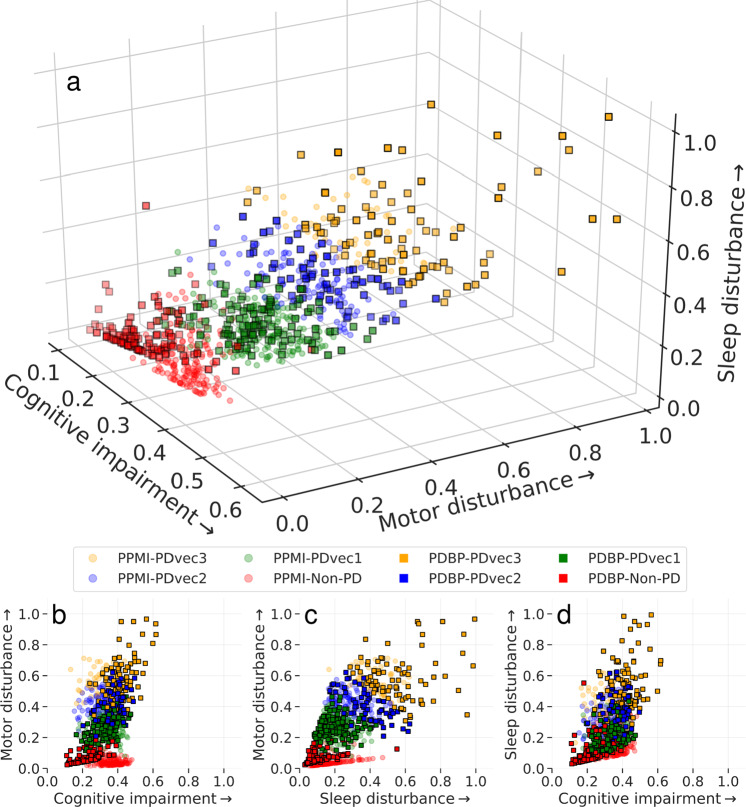
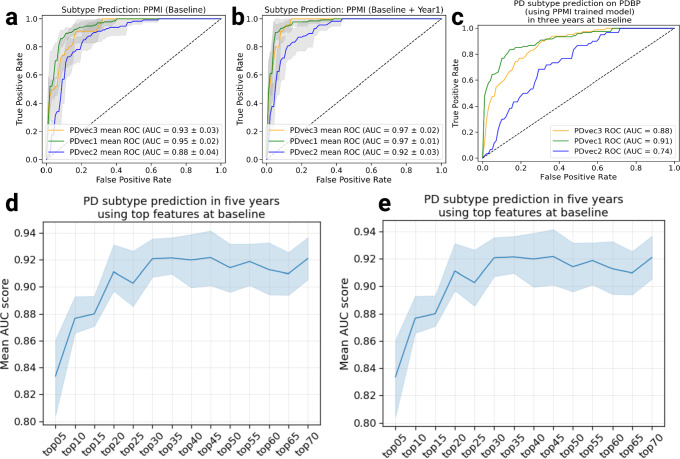
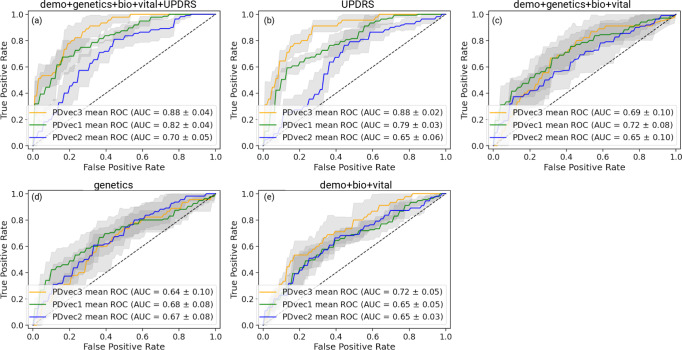
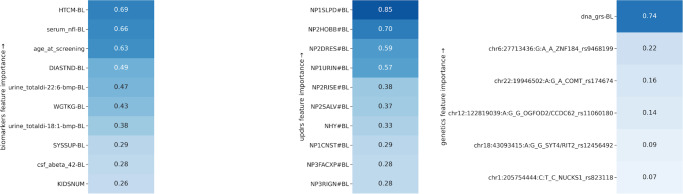
The clinical manifestations of Parkinson's disease (PD) are characterized by heterogeneity in age at onset, disease duration, rate of progression, and the constellation of motor versus non-motor features. There is an unmet need for the characterization of distinct disease subtypes as well as improved, individualized predictions of the disease course. We used unsupervised and supervised machine learning methods on comprehensive, longitudinal clinical data from the Parkinson's Disease Progression Marker Initiative (n = 294 cases) to identify patient subtypes and to predict disease progression. The resulting models were validated in an independent, clinically well-characterized cohort from the Parkinson's Disease Biomarker Program (n = 263 cases). Our analysis distinguished three distinct disease subtypes with highly predictable progression rates, corresponding to slow, moderate, and fast disease progression. We achieved highly accurate projections of disease progression 5 years after initial diagnosis with an average area under the curve (AUC) of 0.92 (95% CI: 0.95 ± 0.01) for the slower progressing group (PDvec1), 0.87 ± 0.03 for moderate progressors, and 0.95 ± 0.02 for the fast-progressing group (PDvec3). We identified serum neurofilament light as a significant indicator of fast disease progression among other key biomarkers of interest. We replicated these findings in an independent cohort, released the analytical code, and developed models in an open science manner. Our data-driven study provides insights to deconstruct PD heterogeneity. This approach could have immediate implications for clinical trials by improving the detection of significant clinical outcomes. We anticipate that machine learning models will improve patient counseling, clinical trial design, and ultimately individualized patient care.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
A.D., H.L., H.I., M.A.N., and F.F.‘s declare no competing non-financial interests but the following competing financial interests as their participation in this project was part of a competitive contract awarded to Data Tecnica International LLC by the National Institutes of Health to support open science research. M.A.N. also currently serves on the scientific advisory board for Character Bio and is an advisor to Neuron23 Inc. The study’s funders had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. Authors V.S., R.K., S.H.H., M.B.M, K.J.B, S.B.C., L.J.S., A.J.N., Ali D., C.B., K.M., S.W.S., A.B.S., and R.H.C. declare no competing financial or non-financial interests. All authors and the public can access all data and statistical programming code used in this project for the analyses and results generation. F.F. takes final responsibility for the decision to submit the paper for publication.
Figures
References
-
- Stebbins GT, et al. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson’s disease rating scale: comparison with the unified Parkinson’s disease rating scale. Mov. Disord. 2013;28:668–670. doi: 10.1002/mds.25383. - DOI - PubMed
Grants and funding
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
LinkOut - more resources
Full Text Sources
