

A multicentric prospective observational study of diagnosis and prognosis features in ICU mesenteric ischemia: the DIAGOMI study
- PMID: 36527517
- PMCID: PMC9759607
- DOI: 10.1186/s13613-022-01092-8
A multicentric prospective observational study of diagnosis and prognosis features in ICU mesenteric ischemia: the DIAGOMI study
Abstract
Background: Non-occlusive mesenteric ischemia (NOMI) is a challenging diagnosis and is associated with extremely high mortality in critically ill patients, particularly due to delayed diagnosis and when complicated by intestinal necrosis. Plasma citrulline and intestinal-fatty acid binding protein (I-FABP) have been proposed as potential biomarkers, but have never been studied prospectively in this setting. We aimed to investigate diagnostic features, the accuracy of plasma citrulline and I-FABP to diagnose NOMI and intestinal necrosis as well as prognosis.
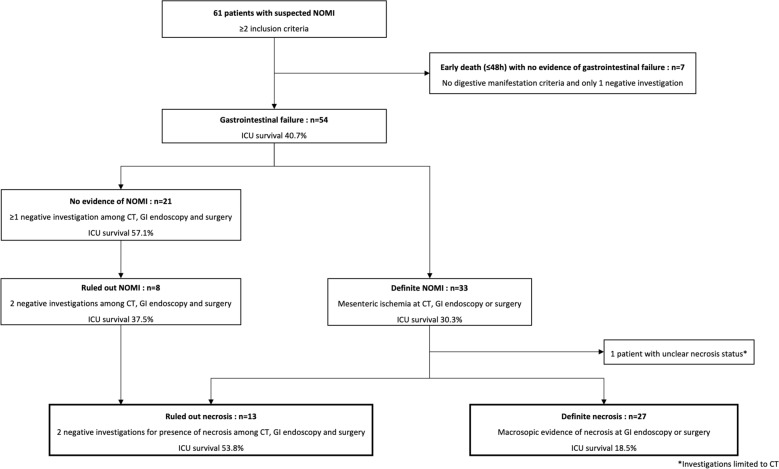
Methods: We conducted a prospective observational study in 3 tertiary ICU centers in consecutive patients with NOMI suspicion defined by at least two inclusion criteria among: new-onset or worsening circulatory failure, gastrointestinal dysfunction, biological signs and CT-scan signs of mesenteric ischemia. Diagnosis features and outcomes were compared according to NOMI, intestinal necrosis or ruled out diagnosis using stringent classification criteria.
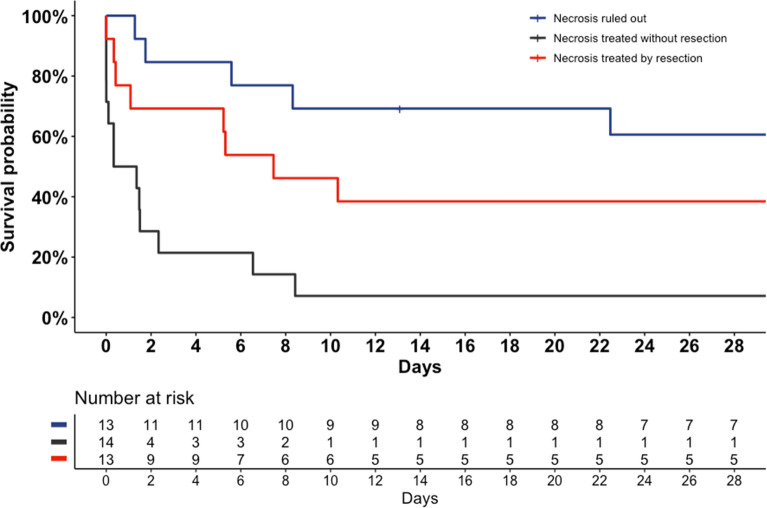
Results: Diagnosis of NOMI was suspected in 61 patients and confirmed for 33 patients, with intestinal necrosis occurring in 27 patients. Clinical digestive signs, routine laboratory results and CT signs of mesenteric ischemia did not discriminate intestinal necrosis from ischemia without necrosis. Plasma I-FABP was significantly increased in presence of intestinal necrosis (AUC 0.83 [0.70-0.96]). A threshold of 3114 pg/mL showed a sensitivity of 70% [50-86], specificity of 85% [55-98], a negative predictive value of 58% [36-93] and a positive predictive value 90% [67-96] for intestinal necrosis diagnosis. When intestinal necrosis was present, surgical resection was significantly associated with ICU survival (38.5%), whereas no patient survived without necrosis resection (HR = 0.31 [0.12-0.75], p = 0.01).
Conclusion: In critically ill patients with NOMI, intestinal necrosis was associated with extremely high mortality, and increased survival when necrosis resection was performed. Elevated plasma I-FABP was associated with the diagnosis of intestinal necrosis. Further studies are needed to investigate plasma I-FABP and citrulline performance in less severe forms of NOMI.
Keywords: Critically ill; Mesenteric ischemia; Observational; Plasma citrulline; Plasma intestinal-fatty acid binding protein.
© 2022. The Author(s).
Conflict of interest statement
Dr Luyt reports having receiving fees from Bayer Healthcare, ThermoFisher Brahms, Biomérieux, Faron, Carmat, Aerogen, Merck Sharp & Dohme, Advanzpharma, outside the submitted work. Dr Pène: Alexion Pharma (institutional grant), GILEAD (consulting and teaching fees).
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
