

Postoperative infections after non-elective cesarean section - a retrospective cohort study of prevalence and risk factors at a single center in Denmark administering prophylactic antibiotics after cord clamping
- PMID: 36528589
- PMCID: PMC9758935
- DOI: 10.1186/s12884-022-05300-y
Postoperative infections after non-elective cesarean section - a retrospective cohort study of prevalence and risk factors at a single center in Denmark administering prophylactic antibiotics after cord clamping
Abstract
Background: Mothers giving birth by non-elective cesarean section have considerably higher risk of developing postoperative infection, than mothers giving birth by elective cesarean section. Meta-analyses have shown that the risk of infection is reduced when administering antibiotics at least 30 min prior to skin incision rather than after cord clamping. If given prior to incision, antibiotics are present in the neonatal bloodstream for up to 24 h after delivery, with early exposure to antibiotics potentially disturbing development of the gut microbiome. We aimed to retrospectively assess the prevalence of postoperative infection after non-elective cesarean section at a single labor ward administering antibiotics after cord clamping, additionally investigating risk factors for developing postoperative infections.
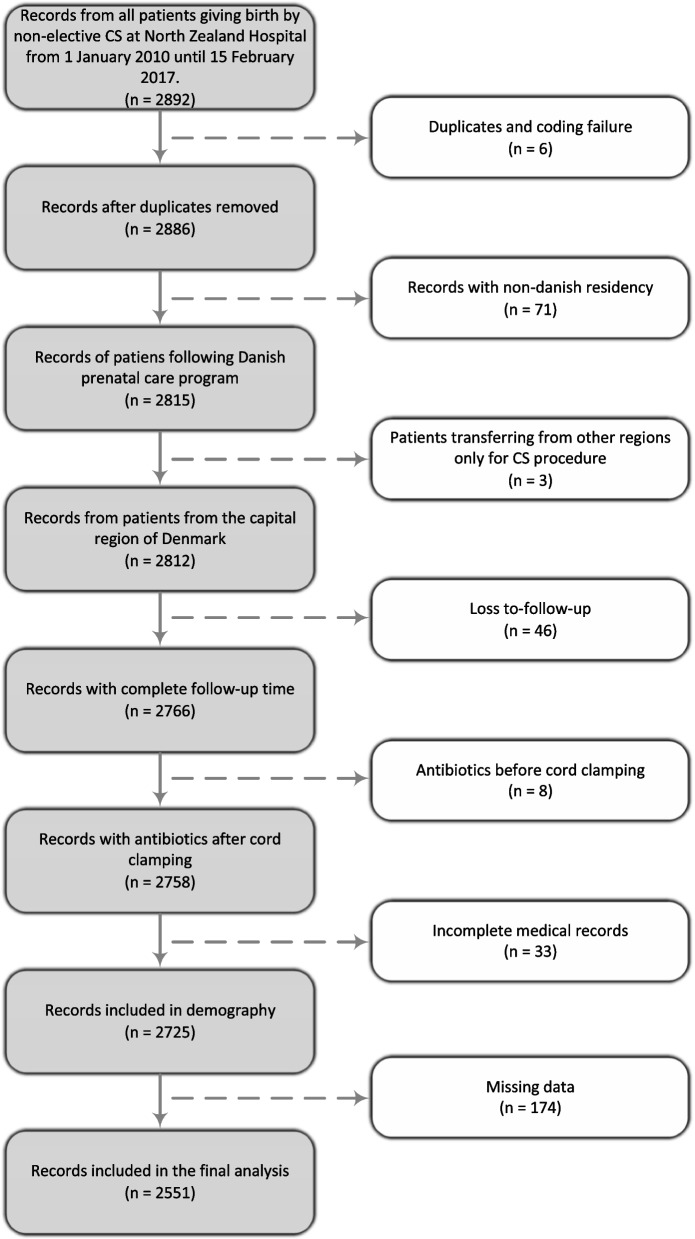
Methods: In this retrospective cohort study, we included a total of 2,725 women giving birth by non-elective cesarean section in 2010-2017 with a review of records for prenatal risk factors, labor management, and perinatal outcomes. The primary outcomes were a main composite infection of development of either endometritis, surgical-site infection, or sepsis in conjunction with a relevant antibiotic prescription. Secondary outcomes included infection of unknown focus, mastitis, urinary tract infection, and pneumonia.
Results: A total of 88 patients developed a main composite infection (3.2%). These infections subdivide into endometritis (n = 37/2725, 1.4%), surgical-site infection (n = 35/2725, 1.3%) and sepsis (n = 15/2725, 0.6%). We found a high body mass index (aOR = 3.38, 95%CI 1.93-5.92) and intrapartum fever (aOR = 2.26, 95%CI 1.22-4.59) to be independent risk-factors for developing postoperative infection after non-elective cesarean section. Furthermore, we found delivery by a more expedient emergency grade 2 cesarean section (aOR = 0.61 95%CI 0.37-0.998) compared to grade 3 to be a protective factor for developing postoperative infection after non-elective cesarean section.
Conclusion: In a labor ward administering antibiotics after cord clamping at non-elective cesarean births, we find a low prevalence of main composite infections when compared to estimates from meta-analyses on the topic. We conclude that administration of prophylactic antibiotics after cord clamping appears to result in acceptable rates of postoperative infection and avoids transplacental-transmission of antibiotics to the infant.
Keywords: Antibiotic prophylaxis/standards; Cesarean section; Guidelines as topic; Puerperal infection/prevention and control; Surgical wound infection/prevention and control.
© 2022. The Author(s).
Conflict of interest statement
All author have no interests to declare.
Figures
Similar articles
-
Comparison of administration of single dose ceftriaxone for elective caesarean section before skin incision and after cord clamping in preventing post-operative infectious morbidity.Arch Gynecol Obstet. 2013 Dec;288(6):1263-8. doi: 10.1007/s00404-013-2906-9. Epub 2013 May 29. Arch Gynecol Obstet. 2013. PMID: 23715925 Clinical Trial.
-
Timing of Antibiotic Prophylaxis in Elective Caesarean Delivery: A Multi-Center Randomized Controlled Trial and Meta-Analysis.PLoS One. 2015 Jul 6;10(7):e0129434. doi: 10.1371/journal.pone.0129434. eCollection 2015. PLoS One. 2015. PMID: 26148063 Free PMC article. Clinical Trial.
-
Antibiotic prophylaxis before surgery vs after cord clamping in elective cesarean delivery: a double-blind, prospective, randomized, placebo-controlled trial.Arch Surg. 2011 Dec;146(12):1404-9. doi: 10.1001/archsurg.2011.725. Arch Surg. 2011. PMID: 22184305 Clinical Trial.
-
Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections.Cochrane Database Syst Rev. 2020 Apr 26;4(4):CD007892. doi: 10.1002/14651858.CD007892.pub7. Cochrane Database Syst Rev. 2020. PMID: 32335895 Free PMC article.
-
Timing of Intravenous Prophylactic Antibiotic Agents for Cesarean Delivery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Surg Infect (Larchmt). 2023 May;24(4):303-310. doi: 10.1089/sur.2022.389. Surg Infect (Larchmt). 2023. PMID: 37126077
Cited by
-
Pneumonia Deterioration Occurring After C-section in a Preeclamptic Patient: A Case Report.Cureus. 2023 Mar 14;15(3):e36147. doi: 10.7759/cureus.36147. eCollection 2023 Mar. Cureus. 2023. PMID: 37065353 Free PMC article.
-
A Predictive Nomogram for Post-Cesarean Infections: Risk Factors and Clinical Implications.Med Sci Monit. 2025 Jul 2;31:e947803. doi: 10.12659/MSM.947803. Med Sci Monit. 2025. PMID: 40598740 Free PMC article.
-
A comprehensive study on the risk factors and pathogen analysis of postoperative wound infections following caesarean section procedures.Int Wound J. 2024 Jan;21(1):e14609. doi: 10.1111/iwj.14609. Int Wound J. 2024. Retraction in: Int Wound J. 2025 Apr;22(4):e70607. doi: 10.1111/iwj.70607. PMID: 38272798 Free PMC article. Retracted.
References
-
- Jyothirmayi CA, Halder A, Yadav B, Samuel ST, Kuruvilla A, Jose R. A randomized controlled double blind trial comparing the effects of the prophylactic antibiotic, Cefazolin, administered at caesarean delivery at two different timings (before skin incision and after cord clamping) on both the mother and newborn. BMC Pregnancy Childbirth. 2017;17(1):1–8. doi: 10.1186/s12884-017-1526-y. - DOI - PMC - PubMed
-
- Ben Shoham A, Bar-Meir M, Ioscovich A, Samueloff A, Wiener-Well Y. Timing of antibiotic prophylaxis in cesarean section: retrospective, difference-in-differences estimation of the effect on surgical-site-infection. J Matern Neonatal Med. 2019;32(5):804–8. doi: 10.1080/14767058.2017.1391784. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
